CISNE Score (Febrile Neutropenia) Calculator: Evidence-Based Triage
An evidence-based guide to using the CISNE score for risk-stratifying stable febrile neutropenia patients with solid tumors.
Quick Navigation
- 1. Introduction to CISNE Score for Febrile Neutropenia
- 2. Defining the CISNE Score
- 3. Clinical Significance of CISNE Score in Practice
- 4. Clinical Evidence and Validation of CISNE
- 5. How the OncoToolkit CISNE Calculator Works
- 6. Linking CISNE Scores to Risk and Management
- 7. Clinical Use Cases for the CISNE Calculator
- 8. Supporting Care, Education, and Research
- 9. Recent Advances and Modifications to CISNE
- 10. Clinical FAQ
1. Introduction to CISNE Score for Febrile Neutropenia
Managing febrile neutropenia (FN) in patients receiving chemotherapy is a daily challenge in oncology and hematology practice. Even in patients who appear clinically stable, a subset will deteriorate rapidly, and distinguishing truly low‑risk cases from those needing close monitoring or admission is not always straightforward.1, 2
The Clinical Index of Stable Febrile Neutropenia (CISNE) score was developed to fill this gap by quantifying the risk of serious complications specifically in patients with solid tumors and apparently stable FN. At OncoToolkit, we have built a CISNE Score (Febrile Neutropenia) calculator that turns this evidence‑based index into an intuitive, mobile‑friendly decision support tool, reducing calculator fatigue for busy clinicians at the bedside or in the emergency department. [2]
2. Defining the CISNE Score
CISNE is a prognostic score designed for adults with solid tumors who present with chemotherapy‑induced FN and are initially hemodynamically stable. It estimates the risk of “serious complications” such as ICU admission, hypotension requiring vasopressors, respiratory failure, acute renal failure, or in‑hospital death.1, 2
The score assigns points to six clinical variables:3, 1
- ECOG performance status ≥ 2 (2 points)
- Chronic obstructive pulmonary disease (1 point)
- Chronic cardiovascular disease (1 point)
- Mucositis ≥ grade 2 (NCI‑CTCAE) (1 point)
- Monocyte count < 200/µL (1 point)
- Stress hyperglycemia or diabetes (1 point)
Total CISNE scores range from 0 to 8 and are grouped into three risk classes with corresponding serious complication rates: [2], [1]
| Risk class | CISNE score | Typical serious complication rate* | | :--- | :--- | :--- | | Low risk | 0 | ≈1–2% | | Intermediate | 1–2 | ≈5–10% | | High risk | ≥3 | ≈30–40% |
*Representative ranges from multicenter validation cohorts; exact rates vary slightly between studies.4, 2
In contemporary guidelines, CISNE complements the older MASCC (Multinational Association for Supportive Care in Cancer) risk index by focusing on the “apparently stable” subgroup, helping clinicians identify which of these patients are truly safe for outpatient management.5, 1
3. Clinical Significance of CISNE Score in Practice
Risk stratification in FN directly informs level of care, need for admission, intensity and route of antibiotics, and follow‑up strategy. Traditional tools such as the MASCC index work well for broad risk assessment, but they may misclassify some “stable” patients who later deteriorate, especially those with subtle organ dysfunction or comorbidities.4, 5, 1
CISNE specifically targets this gray zone, offering:
- A structured way to assess apparently stable FN in solid tumors.
- Better identification of patients at high risk of serious complications despite initial stability. [2], [4]
- Support for decisions regarding early discharge, observation‑unit care, or continued inpatient management in combination with MASCC and clinical judgment.5, 1
Without digital support, calculating CISNE often requires memorizing point assignments, flipping between tables, and cross‑checking risk classes, which is error‑prone during hectic on‑call shifts. By contrast, on our platform the CISNE calculator is responsive on mobile and desktop, optimized for rapid use during MDT huddles, ED triage, or ward rounds, minimizing cognitive load and reducing the risk of overlooking key risk factors.
4. Clinical Evidence and Validation of CISNE
4.1 The Math Behind the CISNE Score
CISNE was originally derived using multivariable logistic regression in a cohort of adults with solid tumors and stable FN. Each of the six predictors was assigned an integer point value proportional to its regression coefficient, resulting in a simple additive score from 0 to 8.3, 1, 2
Conceptually, the model estimates the log‑odds of at least one serious complication as:
logit(p) = beta_0 + sum(beta_i * X_i)
where $X_i$ are the binary predictors (e.g., ECOG ≥ 2, COPD), each with its own coefficient that has been translated into a 1‑ or 2‑point weight. Our calculator faithfully reproduces this point‑based logic: it sums the points for each present factor and maps the total to the corresponding risk class. [2]
4.2 Validation of CISNE in Western Cohorts
The CISNE score was first validated in the FINITE study, a large multicenter European cohort of adults with solid tumors and seemingly stable FN episodes. In this cohort, with a cutoff of ≥3 points for high risk, CISNE achieved:6, 2
- Sensitivity around 78% for major complications
- Specificity around 78%
- Positive predictive value ≈36%
- Negative predictive value ≈96%
Subsequent retrospective and prospective studies in Europe and North America confirmed that CISNE successfully identifies low‑risk patients suitable for outpatient or early‑discharge strategies, and high‑risk patients who benefit from continued inpatient monitoring.7, 8, 4
4.3 Validation of CISNE in Asian Populations
CISNE has also been evaluated in Asian cohorts, including studies from East Asia and the Middle East. In a large single‑center FN registry with over 500 patients, CISNE (using the same 0–8 scale) demonstrated:1, 4
- Higher mean scores in patients with composite adverse outcomes compared with those with favorable courses.
- Significant association between each individual CISNE component and adverse outcomes.
- Good discrimination when compared with MASCC, with improved net reclassification for identifying high‑risk patients.
While absolute complication rates and comorbidity patterns vary between Western and Asian cohorts, the relative performance of CISNE—particularly its ability to identify high‑risk patients among those who appear stable—has been broadly consistent. This cross‑regional validation supports its use in diverse healthcare systems, including centers in Asia, provided clinicians remain mindful of local infection patterns and supportive‑care resources.4, 1
4.4 Performance Comparison: Western vs Asian Cohorts
Across studies, low‑risk (CISNE 0) patients in Western cohorts typically have serious complication rates around 1–2%, whereas high‑risk (≥3) groups reach 30–40%. Asian studies have reported similarly low event rates in score‑0 patients and high event rates in score‑≥3 patients, though intermediate‑risk groups sometimes show slightly higher complication rates, reflecting baseline differences in comorbidity and infection epidemiology.1, 4, 2
These findings suggest that while risk classes are broadly transportable, local calibration—particularly around the threshold for outpatient management—may be appropriate, and many centers combine MASCC and CISNE or adjust cut‑offs slightly to match institutional outcomes.7, 1
4.5 Guideline Endorsements and Practice Statements
Multiple professional bodies now reference CISNE alongside MASCC when discussing outpatient management of FN:
- The joint ASCO/IDSA guideline on fever and neutropenia in adults with cancer mentions CISNE as a validated tool for identifying low‑risk, stable adults with solid tumors who may be candidates for outpatient oral antibiotic regimens.7, 5
- ESMO Clinical Practice Guidelines on FN also highlight the need for risk‑adapted management, noting CISNE as one of the tools developed specifically for apparently stable patients.9, 1
- Emergency medicine and oncology practice statements have discussed CISNE as part of a structured approach to FN triage in the ED, often using MASCC for broad screening followed by CISNE for refinement.10, 1
4.6 Limitations and Clinical Caveats
Thoughtful use of CISNE requires awareness of its boundaries:
- It was derived for adults with solid tumors and seemingly stable FN; its performance in hematologic malignancies, stem cell transplant recipients, or hemodynamically unstable patients is less certain.4, 2
- Most validation cohorts excluded profound organ failure at baseline, so clinicians should not rely solely on CISNE in critically ill or rapidly deteriorating patients.6, 9
- The score does not incorporate microbiological data or local resistance patterns; it should be combined with institutional FN protocols and antimicrobial stewardship guidance.5
On our platform, we surface these caveats alongside the calculator to reinforce that this is a decision support tool, not a substitute for clinical judgment.
5. How the OncoToolkit CISNE Calculator Works
OncoToolkit’s CISNE Score (Febrile Neutropenia) calculator is designed for rapid, transparent use. Clinicians simply select “Yes” or “No” for each of the six criteria, and the tool calculates the total score and risk class in real time.
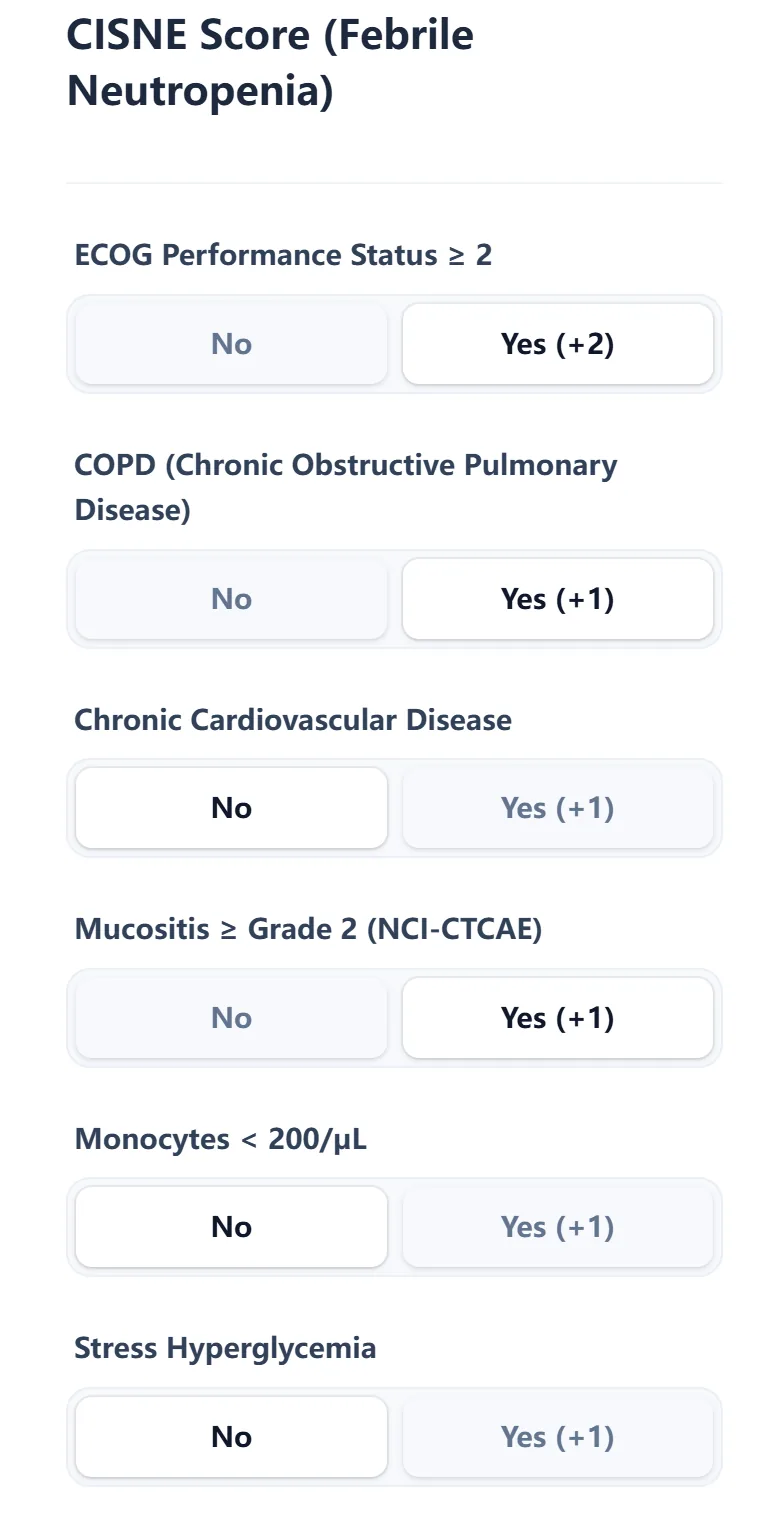
Figure 1. The CISNE calculator input form on OncoToolkit uses simple binary selections for each variable (ECOG performance status, COPD, cardiovascular disease, mucositis, monocytes, and hyperglycemia), minimizing clicks and reducing the chance of missing key risk factors.
Behind the scenes, the algorithm:
- Assigns the appropriate points to each affirmative risk factor (2 points for ECOG ≥2; 1 point for each of the remaining factors).3, 1
- Sums the points into a total CISNE score (0–8).
- Maps the total to the predefined risk class (low, intermediate, or high) and displays an estimated serious complication rate based on pooled validation data.4, 2
The result view emphasizes interpretability:
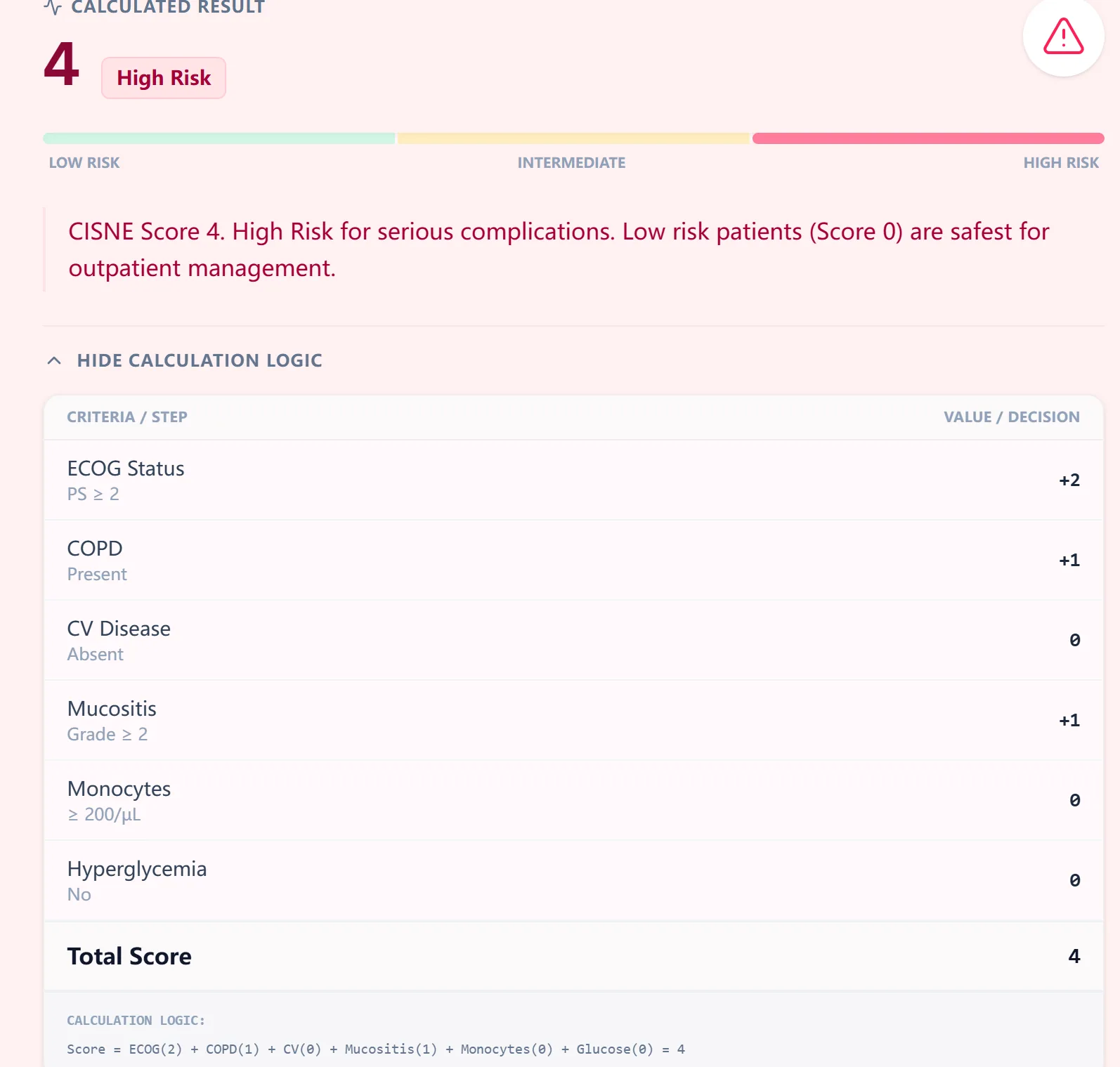
Figure 2. Example CISNE output showing a high‑risk result with a breakdown of how each input contributed to the total score, supporting transparency and resident teaching during FN triage.
Color‑coded bars visually differentiate low, intermediate, and high risk, and an expandable “calculation logic” section shows the point assignment for each criterion so clinicians and trainees can easily follow the reasoning.
6. Linking CISNE Scores to Risk and Management
The calculator also provides a concise reference table that connects CISNE score ranges with observed complication rates.
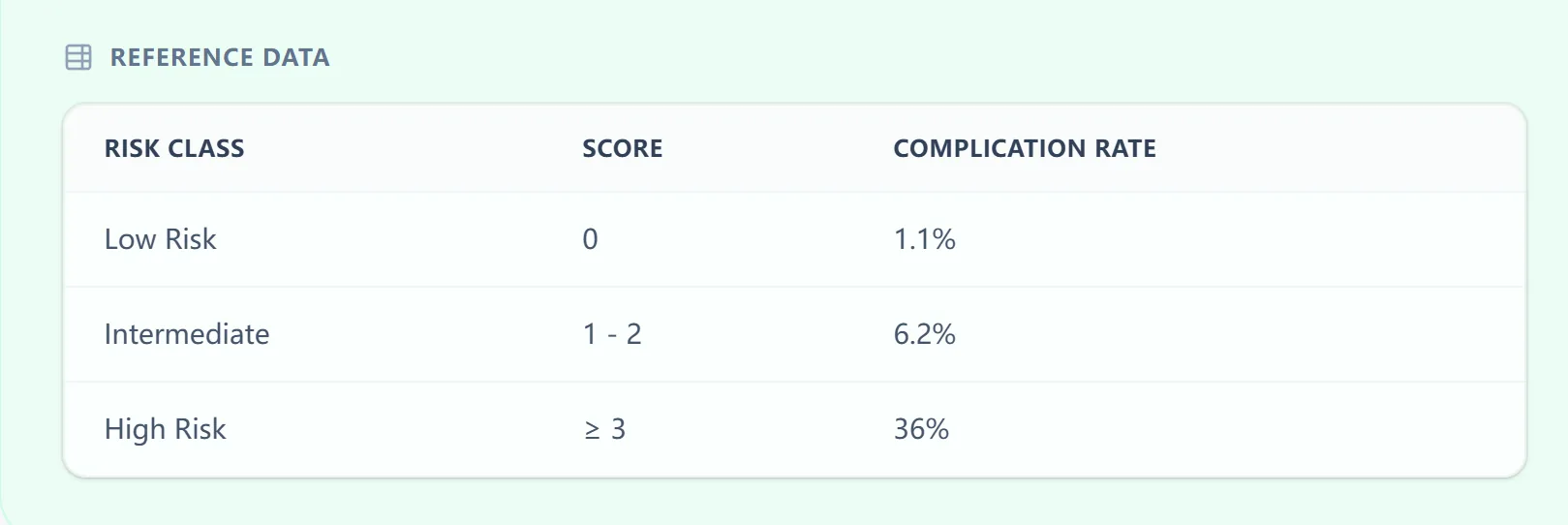
Figure 3. Embedded CISNE reference table summarizing risk classes, score ranges, and expected complication rates to help clinicians rapidly contextualize results during decision‑making.
Typical interpretations might include:5, 1, 2
- Low risk (score 0): Very low probability of serious complications; in appropriate settings, and together with MASCC, patient preference, and social factors, these patients may be candidates for early discharge with oral antibiotics and close follow‑up.
- Intermediate risk (score 1–2): Modest but non‑trivial risk; management often depends on institutional thresholds, comorbidities not captured by CISNE, and logistical factors (e.g., home support, proximity to care).
- High risk (score ≥3): Substantial risk of serious complications; typically warrant inpatient care, careful monitoring, and early escalation of therapy or level of care as needed.
Our calculator pairs each risk class with a succinct management note reminding users that disposition decisions should integrate MASCC scores, guideline recommendations (ASCO/IDSA, ESMO), and clinical judgment rather than relying solely on any single calculator.9, 5
7. Clinical Use Cases for the CISNE Calculator
OncoToolkit’s CISNE calculator is tailored for real‑world workflows across the oncology continuum. Clinically relevant use cases include:
- Emergency department triage of FN: Quickly risk‑stratify adults with solid tumors and apparently stable FN to decide on admission vs observation vs outpatient pathways, alongside MASCC and institutional protocols.10, 5
- Inpatient reassessment: For hospitalized FN patients who remain hemodynamically stable, repeating CISNE can support decisions about step‑down care or early discharge.
- Outpatient oncology clinics: When patients call with fever and recent chemotherapy, pre‑ED assessment with CISNE (once key labs are available) can frame expectations and triage urgency.
- Specialty‑specific oncology (e.g., lung, gynecologic): Sub‑analyses suggest CISNE retains predictive value in disease‑specific populations such as gynecologic cancers and lung cancer, helping identify patients likely to avoid severe FN‑related delays in chemotherapy.8, 7
At OncoToolkit, we have integrated CISNE into a broader “Febrile Neutropenia Triage” panel that also features MASCC and related tools, allowing clinicians to move seamlessly between complementary scores using a consistent interface. This reduces the friction of switching sites and calculators and supports a more holistic, guideline‑concordant triage process. [11], [12]
8. Supporting Care, Education, and Research
Routine Decision Support
The CISNE calculator on our platform is designed for point‑of‑care use:
- Fast data entry optimized for mobile and desktop.
- Immediate score, risk class, and contextual complication rates.
- Clear reminders that recommendations should be integrated with MASCC, guidelines, and clinician judgment.
By centralizing multiple FN tools in one place, OncoToolkit reduces the need to remember separate websites, scoring tables, or apps, thereby lowering cognitive load in high‑pressure environments.
Education and Simulation
For trainees, CISNE offers a structured way to think about risk factors in FN.
Figure 4. The clinical background view within the CISNE calculator summarizes indications, evidence base, and formula logic, making the tool a practical teaching aid for residents and fellows.
Supervisors can:
- Use the calculator during bedside rounds or morning reports to discuss why ECOG status, comorbid COPD or cardiovascular disease, mucositis, monocyte count, and hyperglycemia matter prognostically.
- Demonstrate step‑by‑step how the total CISNE score changes with different patient profiles.
- Reinforce guideline‑based thresholds for outpatient vs inpatient management using real or simulated cases.
Clinical Research and Quality Improvement
Because OncoToolkit uses standardized implementations of widely adopted scores, CISNE can also support research and QI initiatives:
- Cohort‑wide consistency: Applying the same CISNE algorithm across many patients helps ensure consistent risk classification in retrospective audits or prospective registries.1, 4
- Linkage to outcomes: Centers can pair CISNE outputs with local outcomes (e.g., ICU admission, 30‑day mortality, chemotherapy delays) to evaluate whether their cut‑offs for outpatient care remain appropriate.
- Comparative analyses: Combining CISNE with MASCC, Talcott, or institutional scores enables head‑to‑head performance comparisons and recalibration using local data. [13], [6]
9. Recent Advances, Modifications, and Extensions of CISNE
Since its original publication, several groups have explored adjustments and extensions to CISNE:
- Alternative cut‑offs: Some studies in gynecologic oncology and mixed cohorts examined lowering the low‑risk cutoff (e.g., treating scores 0–1 as low risk) to enhance sensitivity, particularly when combined with MASCC, although this may modestly increase unnecessary admissions.7
- Combined strategies (MASCC + CISNE): Work comparing MASCC and CISNE suggests that using MASCC for initial screening and then applying CISNE, sometimes with a lower high‑risk threshold, can optimize both safety and resource use. [13], [7]
- Disease‑specific evaluations: Investigators in lung cancer cohorts have shown that CISNE, along with MASCC, can predict which patients are less likely to experience treatment‑limiting FN episodes, informing chemotherapy scheduling and supportive care strategies. [14], [8]
To date, however, the core six‑variable, 0–8‑point CISNE structure remains intact; there is no universally adopted “CISNE 2.0” with different variables. Instead, advances have focused on refining thresholds, combining CISNE with other scores, and validating its use in broader disease contexts and regions.1, 2
Our implementation on OncoToolkit adheres to the original, guideline‑recognized scoring system while annotating common variations in interpretation (such as institutional preferences around cut‑offs) in the clinical background section.
10. Clinical FAQ
Can the CISNE score be used in patients with hematologic malignancies or unstable FN?
CISNE was derived and validated primarily in adults with solid tumors and seemingly stable FN, explicitly excluding patients with overt organ dysfunction at presentation. In hematologic malignancies, transplant settings, or hemodynamically unstable FN, its performance is less certain; clinicians should rely on broader risk tools, disease‑specific guidance, and ICU criteria rather than CISNE alone.6, 9, 5, 2
How does CISNE differ from the MASCC risk index?
MASCC is a general FN risk index applicable to a wide range of patients, including those with hematologic malignancies, and is widely endorsed in guidelines for identifying low‑risk candidates for outpatient therapy. CISNE, by contrast, is narrower in scope—focusing on apparently stable adults with solid tumors—and incorporates specific comorbidities and laboratory parameters (e.g., ECOG, COPD, mucositis, monocytes, hyperglycemia) to better discriminate high‑risk patients within that “stable” subgroup. Many centers use MASCC for broad triage and CISNE for refinement in eligible patients.5, 2, 1
What is the most common mistake when calculating CISNE?
Common pitfalls include applying CISNE to patients outside its intended population (e.g., hemodynamically unstable, severe organ failure, hematologic malignancies) and misclassifying ECOG performance status or mucositis grade. Using a digital implementation like OncoToolkit’s CISNE calculator, which clearly defines each variable and automates the point assignment, helps reduce these errors.2, 1
Is CISNE validated in both Western and Asian populations?
Yes. CISNE has been validated in multicenter European cohorts and North American datasets as well as in Asian populations, where it continues to discriminate between low‑ and high‑risk patients with stable FN. While some Asian studies suggest slightly different event rates in intermediate‑risk groups, the overall risk gradient and relative performance compared with MASCC are preserved, supporting its global applicability with local calibration.4, 1, 2
When should you not rely solely on CISNE for decision‑making?
Clinicians should avoid relying solely on CISNE when patients are clinically unstable, have significant organ dysfunction at presentation, fall outside the original derivation population, or when local guideline pathways mandate admission regardless of risk score (e.g., lack of outpatient infrastructure). In these situations, CISNE may still inform prognosis but should not override urgent clinical judgment or institutional protocols.9, 5
Ready to Simplify Your FN Triage?
Access our mobile-optimized tool to calculate the CISNE score at the bedside.
Calculate CISNE Score Now
Free to use. No registration required.
References
- PMC Article (12315415): Comprehensive evaluation of CISNE in clinical registries. Source
- Coyne et al. (2015). Validation of the CISNE score for febrile neutropenia. Source
- CancerCalc. CISNE Score point assignments and criteria. Source
- PMC Article (6312365): Multicenter validation of CISNE in diverse cohorts. Source
- IDSA/ASCO Guidelines for Febrile Neutropenia Management. Source
- Journal of Clinical Oncology (FINITE study derivation). Source
- PMC Article (8414105): CISNE and MASCC comparison in clinical settings. Source
- PMC Article (9750814): Disease-specific validation in solid tumors. Source
- ESMO Clinical Practice Guidelines: Febrile Neutropenia. Source
- AAEM Practice Statement for FN Triage in the ED. Source
- OncoToolkit Febrile Neutropenia Triage Panel. Source
- OncoToolkit Home. Source
- PubMed (29168032): Head-to-head performance of MASCC vs CISNE. Source
- Wiley Online Library: CISNE in lung cancer cohorts. Source
- Ovid JCOPR: Global guidelines for FN management. Source
- Prognostic Tools: Clinical CISNE Calculator Reference. Source