1. MIPI (Mantle Cell Lymphoma) Calculator: A Practical Guide for Busy Clinicians
Mantle cell lymphoma (MCL) is an aggressive, biologically heterogeneous B‑cell non‑Hodgkin lymphoma in which individual patient trajectories range from indolent disease to rapidly progressive, treatment‑refractory courses. Treatment choices now span intensive chemo‑immunotherapy, high‑dose cytarabine and autologous transplant, BTK inhibitors, bispecific antibodies, and cellular therapies, making accurate baseline risk assessment essential. At OncoToolkit, we’ve built an online MIPI (Mantle Cell Lymphoma) calculator to make this risk assessment fast, transparent, and easy to integrate into everyday oncology and hematology practice.1, 2, 3, 4, 5, 6
Without digital support, manually applying the Mantle Cell Lymphoma International Prognostic Index (MIPI) requires recalling exact cut‑points, logarithmic transformations, and risk thresholds—an unrealistic expectation in busy clinics, day units, and MDTs. On our platform, this calculator automates the math, provides instant risk categorization with estimated survival, and reduces “calculator fatigue” so clinicians can focus on nuanced decisions such as transplant eligibility, trial referral, or the timing of novel agents.2, 7, 1
2. What is the MIPI Score?
The Mantle Cell Lymphoma International Prognostic Index (MIPI) is a validated prognostic model developed for patients with advanced‑stage MCL using data from 455 patients enrolled in prospective trials of first‑line immunochemotherapy. It combines four routinely available variables—age, Eastern Cooperative Oncology Group (ECOG) performance status, serum lactate dehydrogenase (LDH) level relative to the upper limit of normal (ULN), and leukocyte (WBC) count—to generate a continuous prognostic score that is grouped into discrete risk categories.7, 1, 2
Historically, generic scores such as the International Prognostic Index (IPI) did not adequately distinguish outcomes among patients with MCL, especially across low‑ and intermediate‑risk strata. The development of MIPI addressed this gap and demonstrated superior prognostic performance compared with IPI in cohorts treated with intensive first‑line rituximab‑based immunochemotherapy plus autologous stem cell transplant. In the original analysis, low‑risk patients (approximately 44% of the cohort) had a median overall survival (OS) that was not reached, intermediate‑risk patients had a median OS of about 51 months, and high‑risk patients had a median OS of around 29 months. These clear gradients in survival underpin the enduring relevance of MIPI in both clinical practice and research.8, 9, 10, 1, 2, 7
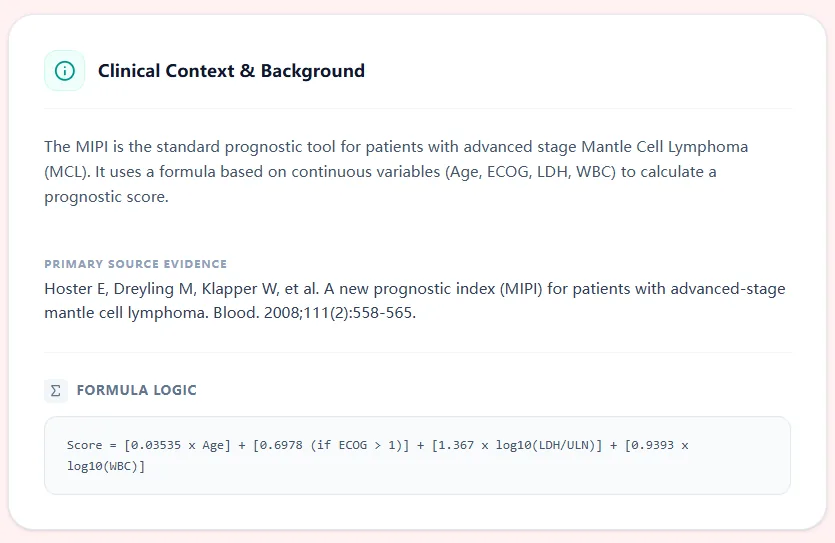
Figure 1. The clinical context panel in our MIPI calculator summarizes how the index was developed, which variables are required, and what outcomes it predicts.
3. Why the MIPI Score Matters in Practice
3.1 How MIPI Guides Treatment Decisions
For oncologists and hematologists, accurately defining MCL risk at diagnosis and at critical decision points has direct therapeutic implications.3, 11, 12, 13
Choice of frontline intensity. ESMO guidelines (endorsed by EHA) and the 2025 EHA–EU MCL Network guidance both recognize MIPI as a key tool for baseline risk assessment when selecting between intensive cytarabine‑containing regimens with autologous transplant and less‑intensive or targeted approaches. Low‑risk, fit patients may be steered toward intensive strategies, whereas high‑risk or frail patients are candidates for less intensive, novel‑agent‑focused or trial‑based strategies.4, 11, 12
Eligibility and stratification for transplant and cellular therapy. In cohorts undergoing high‑dose therapy and autologous transplant, MIPI identifies patients with particularly favorable or unfavorable outcomes and is often used to stratify arms in trials and registries.5, 9, 10
Counseling on prognosis and follow‑up intensity. Clear prognostic categories support transparent discussions with patients about expected survival, inform surveillance schedules, and guide the intensity of supportive care.14, 1, 3
3.2 Reducing Cognitive Load with Digital Support
In practice, clinicians often juggle multiple prognostic schemes, including MIPI, simplified MIPI (s‑MIPI), combined indices that incorporate Ki‑67 (MIPI‑c), and evolving gene‑expression or immune scores. Carrying these in memory, alongside various disease‑specific algorithms and guideline nuances, contributes to cognitive overload. On our platform, the MIPI (Mantle Cell Lymphoma) calculator is mobile‑responsive and optimized for rapid use during MDTs, teleconferences, or bedside reviews, so you can generate a clearly labeled risk group and survival estimate in seconds, with no need to consult printed tables or separate apps.15, 16, 3
4. Clinical Evidence and Validation
4.1 The Math Behind the MIPI Calculator
MIPI is built on a Cox proportional hazards model that treats age, LDH ratio (LDH/ULN), and WBC count as continuous variables, while ECOG performance status enters as a categorical term. The continuous score implemented in our calculator uses the standard published coefficients:17, 1, 2
Score = 0.03535 x Age + 0.6978 x I(ECOG > 1) + 1.367 x log10(LDH / ULN) + 0.9393 x log10(WBC)
This linear predictor is then mapped to three risk categories: low risk for scores < 5.7, intermediate risk for 5.7-6.2, and high risk for >= 6.2. On our platform, both the numerical value and categorical risk group are displayed, ensuring transparency for advanced users while maintaining simplicity for trainees.18, 7
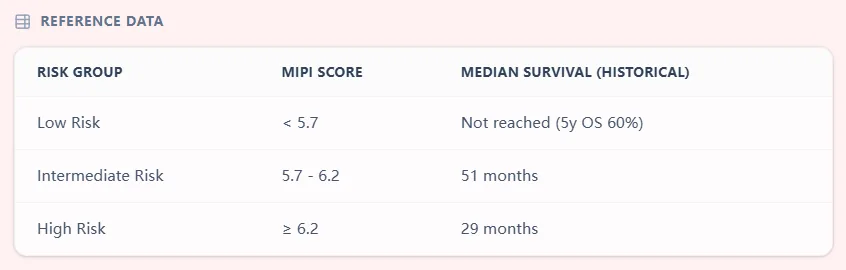
Figure 2. The reference data table in our calculator shows how continuous MIPI scores translate into low‑, intermediate‑, and high‑risk groups, with historical median overall survival estimates drawn from the original studies.
4.2 Validation Across Treatment Eras
The original derivation and validation studies demonstrated that MIPI robustly stratifies survival across different treatment intensities, including CHOP‑like regimens and more intensive cytarabine‑containing protocols. Subsequent independent validations confirmed its prognostic value in real‑world cohorts, transplant series, and intensive immunochemotherapy settings, with MIPI outperforming IPI in predicting survival after high‑dose therapy and autologous stem cell transplant.9, 10, 19, 1, 2
As treatment paradigms evolved to include bendamustine‑based regimens, BTK inhibitors, and combinations with anti‑CD20 antibodies, analyses from North American and European consortia showed that MIPI still retains independent prognostic significance, although additional variables (e.g., Ki‑67, TP53 status, metabolic tumor volume) further refine risk discrimination. Contemporary reviews stress that MIPI remains a foundational “backbone” score against which newer models are compared.20, 3, 4, 14, 15
4.3 Guideline Recommendations
International guidelines have incorporated MIPI into routine practice recommendations:
- EHA/ESMO guidelines for newly diagnosed MCL (2020 endorsement). These guidelines endorse the use of MIPI at baseline to define low‑ versus high‑risk populations and to inform treatment intensity and trial design.11
- EHA–EU MCL Network guidelines (2025). The network guidelines highlight MIPI and its biologic extensions (MIPI‑b, MIPI‑c) as key tools for risk stratification, recommending that risk category be documented systematically in clinical records and used for trial stratification and outcome reporting.12
- NCCN Guidelines for B‑cell Lymphomas (2024 version). NCCN notes that clinical factors summarized by MIPI, along with proliferation index and genetic risk, should be considered when individualizing therapy and counseling.6, 13
4.4 Limitations and Caveats
- Trial‑based derivation. The original cohorts were composed largely of fit patients enrolled in clinical trials, which may underestimate the influence of comorbidities, frailty, or competing mortality.1, 2, 8
- Biologic heterogeneity. MIPI does not include proliferation indices (e.g., Ki‑67), TP53 aberrations, or complex karyotype, all of which have substantial prognostic impact in modern series.16, 3, 15, 20
- Dynamic risk. MIPI is a static baseline index and does not capture response‑adapted risk or changes in molecular status over time; emerging models incorporate treatment response, minimal residual disease, or immune features to provide dynamic prognostication.21, 3, 5, 15
5. Specific Use Cases for the MIPI Calculator
5.1. Staging and Documenting Risk at Diagnosis
At the time of initial MCL diagnosis, clinicians can use our MIPI calculator to generate standardized risk categories for clinic letters, support treatment rationale (intensive vs. targeted), and benchmark patient risk against published cohorts.13, 6, 11, 2, 1
5.2. Pre‑transplant and Intensive Therapy Assessment
Before high‑dose regimens and autologous transplant, MIPI helps identify patients who derive long‑term benefit from upfront intensive strategies or highlight high‑risk cases where toxicity must be weighed against clinical trial or cellular therapy options.10, 9, 5, 14
5.3. Trial Screening and Stratification
Investigators can quickly confirm eligibility for MCL trials that use MIPI categories for stratification, ensuring uniform assignment to risk strata and reducing misclassification during randomization.3, 4, 15, 2
6. How our MIPI Calculator Works
On our platform, the MIPI calculator is designed to mirror real clinical workflows while minimizing data‑entry friction.
1. Tool selection. From the hematology toolbox, the user selects “MIPI (Mantle Cell Lymphoma)” to open a dedicated interface.
2. Input of required variables. Age in years, ECOG performance status (0–1 vs >1), Serum LDH (U/L) and laboratory‑specific ULN, and WBC count (×10⁹/L).
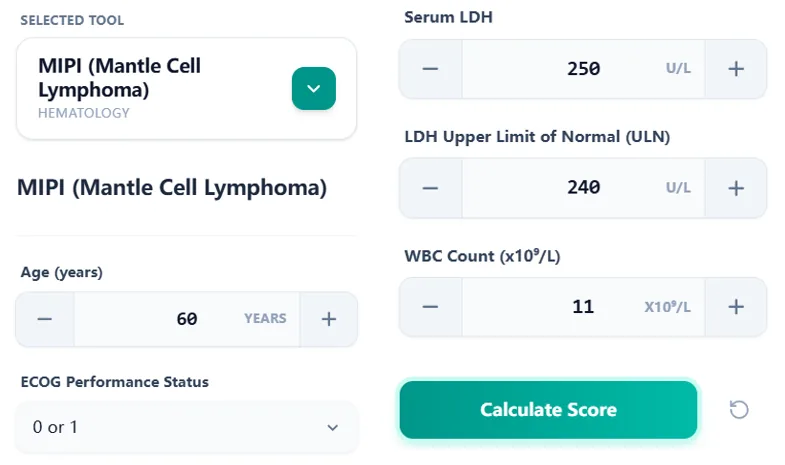
Figure 3. The input form accepts clinical variables with clear unit labels to reduce errors during bedside or MDT use.
3. Computation and quality checks. When the user clicks “Calculate Score”, the tool applies range checks and computes the continuous MIPI using validated coefficients.2
4. Presentation of results. The result card shows the numerical MIPI score, the categorical risk group (color‑coded), and approximate historical median OS with a 5‑year OS estimate.7, 1, 2
Figure 4. The result view facilitates quick documentation in clinic letters, discharge summaries, and MDT minutes.
7. Beyond the Original MIPI: Updates and Extensions
7.1 Simplified MIPI (s‑MIPI)
A version that categorizes variables into discrete risk bands. It offers less granularity but is easier to derive manually.1, 3, 14
8. How OncoToolkit Supports Clinical Care, Education, and Research
8.1. Routine Clinical Decision Support: Standardizes baseline documentation and drives MDT discussion when weighing frontline intensity and transplant.11, 12, 4, 3
8.2. Education and Trainee Simulation: Demonstrates variable influence on risk category shifts and allows simulation of risk-adapted management.2, 13, 12, 11
8.3. Research, Registries, and Quality Improvement: Facilitates registry-level analyses, prospective trial stratification, and quality tracking for high-risk interventions.19, 15, 3, 5, 14
9. Clinical FAQ: MIPI in Real-World Practice
When should you not use the MIPI score?
MIPI is best validated in adults with advanced‑stage MCL receiving first‑line systemic therapy and may be less reliable in localized disease or heavily pre‑treated patients.8, 13, 1, 11, 3, 2
How does MIPI compare with IPI and newer models?
MIPI provides superior prognostic discrimination compared with IPI. However, newer models such as MIPI‑c, Ki‑67‑integrated scores, AMOS, and immune‑based signatures can further refine risk assessment.10, 12, 21, 22, 3
What is the most common mistake when calculating MIPI?
Common manual errors include mis‑scoring ECOG, failing to normalize LDH values to the laboratory’s ULN, and entering WBC in incorrect units. The OncoToolkit calculator minimizes these pitfalls.23, 18, 7, 1
10. Integrate the MIPI Calculator into Your Workflow
To integrate MIPI into your MCL workflow, open our dedicated tool at the link below. We recommend bookmarking the calculator or pinning it to your mobile home screen so that it is always one tap away in clinic, day‑case units, or MDT rooms. Try applying the calculator to several recent MCL cases to see how the risk group and survival estimates shift, and use the interpretation text to standardize your documentation.
Ready to Simplify Your MCL Risk Stratification?
Calculate MIPI scores and access evidence-based survival estimates in seconds.
Use the Calculator Now
FREE TO USE • NO REGISTRATION REQUIRED
References
- Hoster, E., et al. A new prognostic index (MIPI) for patients with Mantle Cell Lymphoma. Blood. 2008. Source
- Hoster, E., et al. MIPI for patients with advanced MCL. Blood Journal. Source
- Mantle Cell Lymphoma: Evolving Management Paradigms. Source
- ASCO Educational Book. Clinical Management of MCL. Source
- Relapsed/Refractory MCL and Novel Therapies. PMC. Source
- NCCN Guidelines Update 2024: B-Cell Lymphomas. Source
- Mantle Cell Lymphoma International Prognostic Index (MIPI). Standard of Care. Source
- Clinical Challenges in MCL Prognostication. PMC. Source
- MIPI vs IPI in Intensive First-Line Immunochemotherapy. Academia. Source
- Outcomes following intensive first-line therapy in MCL. ScienceDirect. Source
- ESMO Guidelines: Newly Diagnosed and Relapsed MCL. PMC. Source
- EHA–EU MCL Network Guidelines 2025. PMC. Source
- NCCN Clinical Practice Guidelines: B-Cell Lymphomas 2024. Source
- Prognostic Indicators for Mantle Cell Lymphoma. OncLive. Source
- Prognostic Scores in Modern MCL Practice. PMC. Source
- Combined MIPI (MIPI-c) and Proliferation Index. JCO. Source
- Standardized Coefficients for MIPI. PubMed. Source
- MIPI Clinical Score Implementation. OmniCalculator. Source
- Validation of MIPI in Independent Cohorts. Blood. Source
- Biological markers and MIPI in MCL. Wiley. Source
- Immune Gene Signatures in MCL 2026. PMC. Source
- AMOS: Integrative Models for MCL. PMC. Source
- Clinical Calculation Safety: Avoiding MIPI Errors. Source