G8 Screening Tool Calculator: Practical Geriatric Oncology Support
Managing older adults with cancer is inherently complex. Chronological age rarely reflects physiologic reserve, multimorbidity is common, and treatment toxicity can be severe if vulnerability is overlooked.
Quick Navigation
- 1. G8 Screening Tool: Practical Geriatric Oncology Support
- 2. What is the G8 Screening Tool?
- 3. Why the G8 Screening Tool Matters in Practice
- 4. Clinical Evidence and Validation
- 4.1. The Math Behind the Tool
- 4.2. Validation Across Western and Asian Populations
- 4.3. Guideline Recommendations and Latest Advances
- 5. How the OncoToolkit G8 Screening Tool Calculator Works
- 6. Clinical Context, Background, and Transparency
- 7. Specific Use Cases for the OncoToolkit G8 Calculator
- 8. How the Platform Supports Education and Research
- 9. Recent Expansions and Modifications of the G8
- 10. Clinical FAQ
- 11. Conclusion: Integrate the G8 Calculator Into Your Workflow
1. G8 Screening Tool: Practical Geriatric Oncology Support
Managing older adults with cancer is inherently complex. Chronological age rarely reflects physiologic reserve, multimorbidity is common, and treatment toxicity can be severe if vulnerability is overlooked. The G8 Screening Tool calculator helps oncologists rapidly flag older patients who may benefit from a full Comprehensive Geriatric Assessment (CGA) before making chemotherapy or immunotherapy decisions. [1], [2]
At OncoToolkit, we’ve built an online G8 Screening Tool calculator that turns this validated questionnaire into a streamlined digital workflow for busy clinics. On our platform, the eight questions, scoring logic, and interpretation thresholds are embedded into a mobile‑friendly interface, reducing cognitive load and “form fatigue” during geriatric oncology consultations. [3]
2. What is the G8 Screening Tool?
The G8 Screening Tool (Geriatric 8) is an eight‑item questionnaire derived from the Mini Nutritional Assessment (MNA) and basic demographic data. It was developed specifically to screen older adults with cancer (typically ≥65–70 years) for geriatric impairments that predict intolerance to standard oncologic therapy and worse outcomes. [4], [2], [5]
The eight items cover:
Each response is assigned a point value; the total G8 score ranges from 0 (most impaired) to 17 (not impaired). A widely used cut‑off is ≤14 to define an abnormal or “impaired/vulnerable” result that should trigger a full CGA, whereas 15–17 usually indicates a “fit” patient suitable for standard oncologic care without mandatory geriatric work‑up. [6], [1], [5]
Since its first evaluation in the ONCODAGE project, the G8 Screening Tool has become one of the most widely studied geriatric oncology screening instruments and is referenced in multiple international recommendations on the management of older adults with cancer. [2], [7], [1]
3. Why the G8 Screening Tool Matters in Practice
Older patients represent a growing proportion of oncology clinics, yet comprehensive geriatric assessment for every patient is not feasible in most settings. The G8 helps prioritize who needs that in‑depth assessment by identifying those with nutritional risk, functional limitations, cognitive concerns, or polypharmacy that might not be obvious from performance status alone. [1], [4], [2]
In practice, using the G8 Screening Tool supports:
- •Treatment planning – Abnormal scores are associated with higher rates of chemotherapy toxicity, unplanned hospitalizations, early treatment discontinuation, and poorer overall survival. [8], [9], [4]
- •Shared decision making – By making vulnerability explicit, the G8 provides a structured way to discuss goals of care, dose adjustments, or alternative regimens that align with patient priorities. [10]
- •Resource allocation – It helps geriatric oncology teams triage referrals for full CGA to those most likely to benefit, rather than working on a first‑come basis. [7], [1]
Without digital support, scoring the G8 requires referencing a paper chart, checking point values for each response, summing them correctly, and remembering the cut‑off. On our platform, the calculator handles scoring and interpretation automatically, is fully mobile‑responsive, and is optimized for use during MDT meetings, pre‑operative assessments, and point‑of‑care rounds. [3]
4. Clinical Evidence and Validation
4.1. The math behind the tool
Mathematically, the G8 is a point‑based weighting system rather than a regression equation. Each of the eight items has 2–4 possible responses with pre‑assigned integer scores; these are summed to produce a total between 0 and 17. Age, nutritional status (food intake, weight loss, BMI), mobility, neuropsychological status, polypharmacy, and self‑rated health each contribute differently, reflecting their relative importance for geriatric vulnerability. [5], [6]
Original development and validation studies used receiver operating characteristic (ROC) analysis to compare different cut‑offs against a reference standard of “abnormal CGA.” A threshold of ≤14 balanced sensitivity (≈85–90%) and specificity (≈55–60%) across multiple cohorts, leading to its widespread adoption as the standard cut‑off. Our calculator implements this sum‑and‑threshold logic exactly: total score ≤14 is flagged as impaired/vulnerable, while 15–17 is considered normal/fit. [9], [2], [1]
4.2. Validation across Western and Asian populations
In Western cohorts, early prospective work showed that the G8 had the highest sensitivity and good specificity among 17 screening tools for predicting abnormal CGA in older cancer patients. In the ONCODAGE project and related studies, around 80% of older adults with advanced solid tumors had an impaired G8 (≤14), and this threshold accurately identified those with abnormal CGA findings. [2], [1]
Subsequent prospective evaluations in Europe demonstrated that impaired G8 scores predicted:
- Shorter overall survival in older patients with lung cancer and other solid tumors treated with chemotherapy. [8], [4]
- Higher risk of severe treatment‑related toxicity and early chemotherapy discontinuation. [9], [10]
- Increased likelihood of functional decline after treatment. [10]
Asia‑Pacific data have grown rapidly in recent years. A prospective study in elderly lung cancer patients in Japan confirmed that abnormal G8 scores were independent predictors of poor overall survival and low relative dose intensity, similar to findings in Western cohorts. Multi‑ethnic Asian data from the GOLDEN study showed that the G8 performed well in identifying older adults who would benefit from CGA, but suggested a slightly lower cut‑off of 13 might further improve sensitivity and specificity in Asian practice. Cross‑cultural adaptation and validation of a Chinese version (C‑G8) also demonstrated acceptable reliability and validity in hospitalized older adults with cancer. [11], [12], [4]
Key Takeaways:
- Western populations: G8 ≤14 robustly identifies patients with abnormal CGA and worse survival.
- Asian populations: G8 retains prognostic value, but some cohorts favor a cut‑off of 13 to better reflect local patient characteristics.
4.3. Guideline recommendations and latest advances
A task force from the International Society of Geriatric Oncology (SIOG) concluded that G8 showed the highest combined sensitivity and specificity among geriatric screening tools for predicting abnormal CGA, and recommended that all cancer patients aged ≥65 undergo screening with tools such as G8 or VES‑13, followed by CGA for those with abnormal results. Contemporary guideline summaries and educational resources, including eviQ and national geriatric oncology pathways, similarly endorse G8 as a first‑line screen before CGA. [6], [7], [1]
More recent reviews highlight that the G8 is not only a CGA gatekeeper but also a prognostic marker for overall and progression‑free survival, including in patients receiving modern therapies such as immune checkpoint inhibitors. Studies in urothelial carcinoma and lung cancer treated with immunotherapy have shown that frail patients identified by low G8 scores experience significantly worse survival, supporting its use in contemporary decision‑making. [13], [14], [4], [8]
5. How the OncoToolkit G8 Screening Tool Calculator Works
On our platform, the G8 Screening Tool calculator reproduces the full eight‑item questionnaire in a clean, touch‑friendly layout. Each item is presented with drop‑down response options that already include the associated point value, so clinicians never need to memorize the scoring scheme.
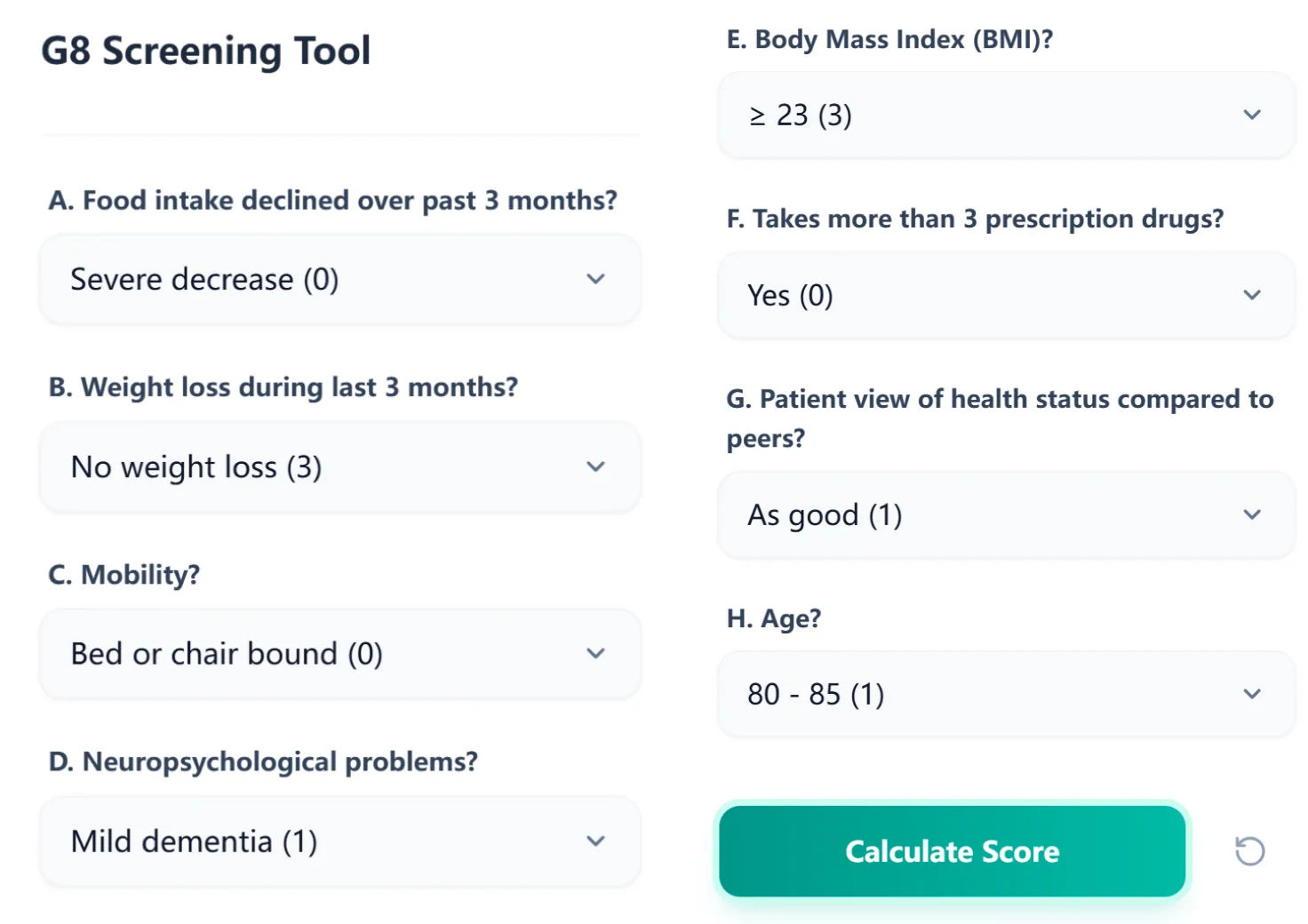
Figure 1. The input screen displays all eight G8 domains—nutrition, weight loss, mobility, cognition, BMI, polypharmacy, self‑rated health, and age—with clearly labeled options and embedded point values, streamlining completion during clinic visits.
To use the calculator, the clinician:
- Selects the appropriate response for each of the eight questions.
- Clicks Calculate Score to generate the total score.
The algorithm sums the points for all eight items (0–17) and then automatically categorizes the result based on standard thresholds:
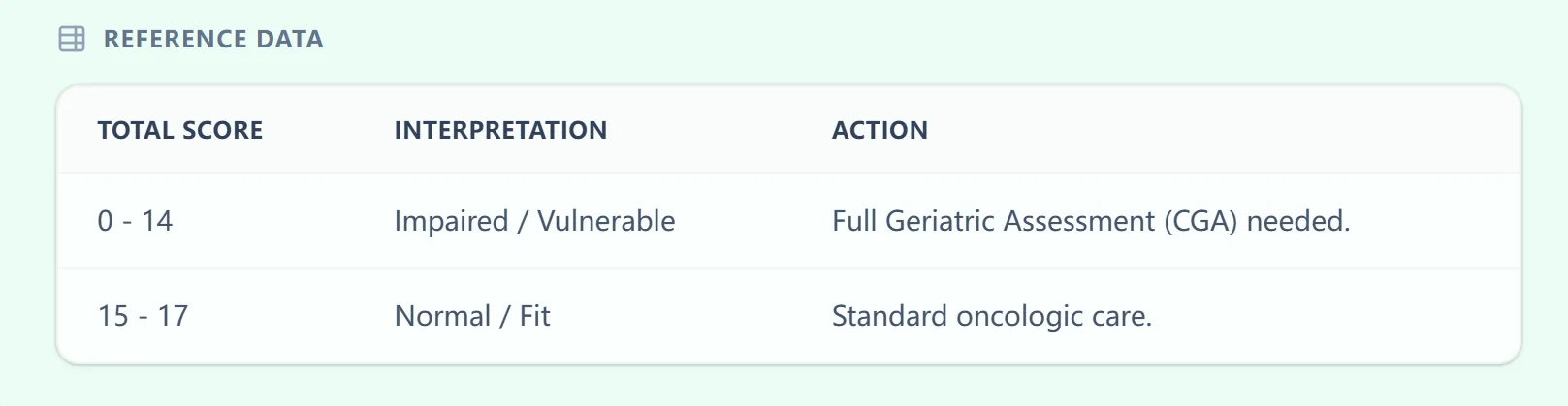
Figure 2. The embedded reference table links total G8 score ranges to interpretation and suggested action, reinforcing standard thresholds and promoting consistent triage to CGA.
The results page provides a clear textual conclusion, such as “Patient is vulnerable. Full Comprehensive Geriatric Assessment (CGA) is indicated,” along a color‑coded bar that visually communicates risk level.
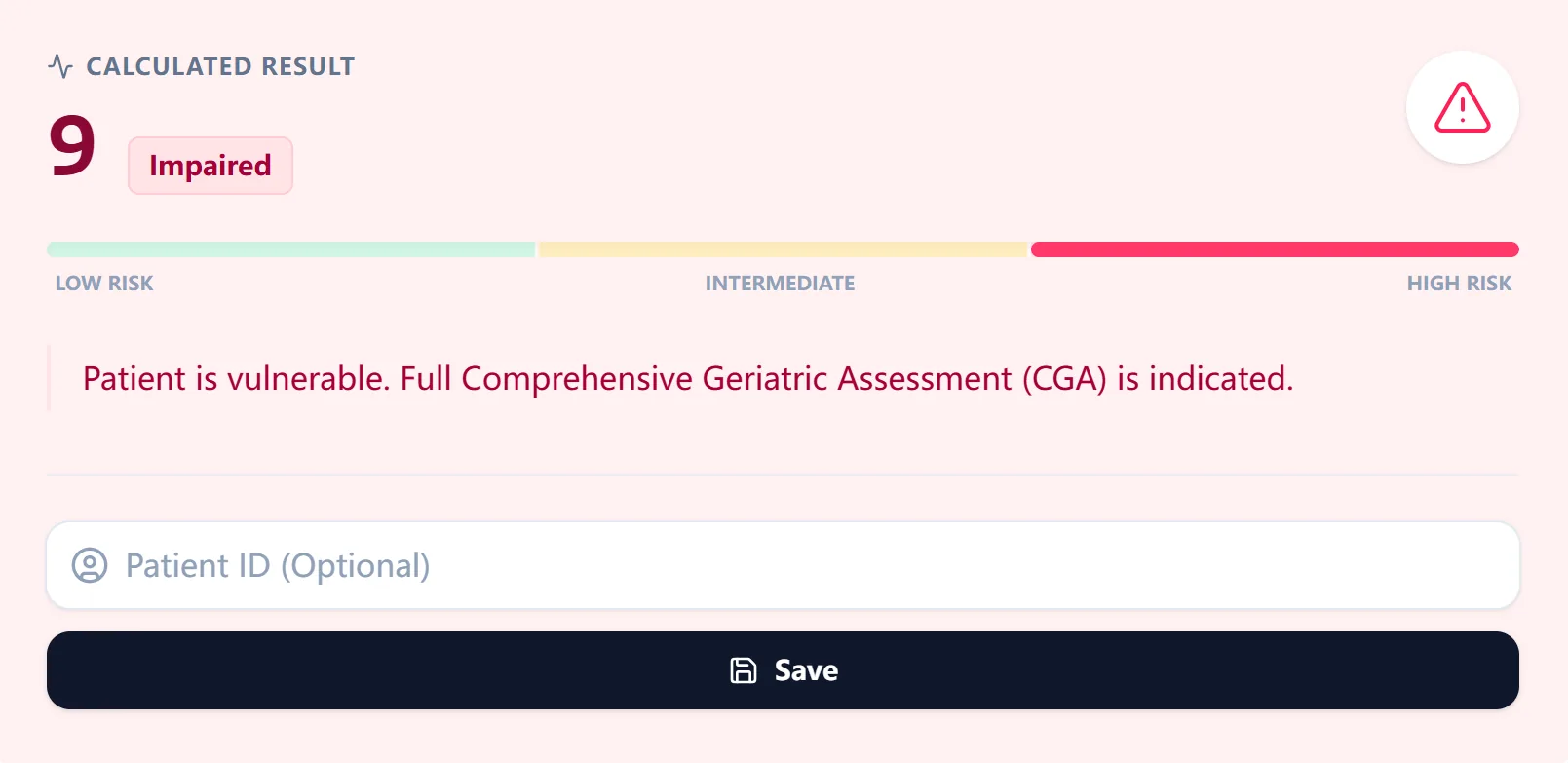
Figure 3. The results view summarizes the total score and vulnerability status, alongside an explicit recommendation regarding CGA, making it easy to understand and document in the medical record or MDT notes.
6. Clinical Context, Background, and Transparency
The calculator also includes a concise Clinical Context & Background panel summarizing how the G8 was derived from the Mini Nutritional Assessment, why a low score indicates vulnerability, and the primary evidence that underpins its use in oncology. [2], [5]
Figure 4. The background panel briefly explains the origin of the G8, cites its first evaluation in older cancer patients, and restates the formula logic.
7. Specific Use Cases for the OncoToolkit G8 Calculator
OncoToolkit’s implementation of the G8 supports several concrete clinical applications:
- New patient consults – Quickly screen adults ≥65–70 years to decide who needs CGA before starting systemic therapy or radical radiotherapy. [15], [1]
- Pre‑operative risk stratification – Combine G8 results with surgical risk tools to identify frail patients for prehabilitation. [16], [1]
- MDT and boards – Record G8 scores to bring objective data into discussions about dose intensity. [16], [10]
- Follow‑up – Use repeat G8 assessments to monitor functional decline or recovery over time. [10]
8. How the Platform Supports Education and Research
For trainees, the G8 calculator demonstrates how core geriatric domains influence oncology decisions and highlights the gap between ECOG performance status and true physiologic reserve. The tool allows “what‑if” simulations during teaching sessions to illustrate how subtle changes can shift a patient from “fit” to “vulnerable.” [4], [1]
From a research and quality‑improvement perspective, saving G8 scores with patient IDs enables:
Service Evaluation
Quantify screening penetration and the proportion of vulnerable patients.
Outcomes Analysis
Link baseline G8 categories to toxicities, hospitalizations, and survival.
Model Comparison
Investigate whether alternative cut‑offs provide better calibration locally.
9. Recent Expansions and Modifications of the G8
Several developments have refined or extended the original G8:
- Modified six‑item G8 – A large prospective European cohort study developed an optimized six‑item version that maintained high sensitivity (≈89%) and improved specificity (≈79%). [17], [9]
- Region‑specific adaptations (C‑G8) – A Chinese cross‑cultural adaptation (C‑G8) confirmed validity and reliability in Mandarin‑speaking settings. [11]
- Alternative cut‑offs in Asian practice – The GOLDEN study found that a cut‑off of 13 performed better than 14 for identifying patients who benefit from CGA. [12]
- New prognostic applications – Recent studies have shown that baseline G8 predicts survival among patients treated with immune checkpoint inhibitors. [14], [13], [4]
10. Clinical FAQ
Clinical Pearl
The G8 is a screening instrument and should not replace a full CGA or detailed clinical assessment when major concerns are present. In patients with obvious frailty, clinicians should proceed to CGA regardless of the G8 score.
How does the G8 compare with other geriatric screening tools?
Compared with instruments such as VES‑13, the G8 is shorter, cancer‑specific, and heavily weighted toward nutritional status. A SIOG task force found that G8 had the best combination of sensitivity and specificity among 17 tools. [5], [1]
Is the G8 validated for Western and Asian populations?
Yes. Western studies demonstrate that G8 ≤14 strongly predicts abnormal CGA and higher toxicity. Asian cohorts confirm prognostic value but sometimes favor a slightly lower cut‑off (13) or adapted versions such as C‑G8. [11], [9], [4], [12], [1]
Does a normal G8 score mean a patient is “fit” for any cancer therapy?
No. A normal G8 (15–17) suggests that a full CGA is unlikely to reveal major impairments, but it does not guarantee tolerance of any regimen. Tumor stage, organ function, and patient goals still need to be weighed carefully. [8], [9]
11. Conclusion: Integrate the G8 Calculator Into Your Workflow
To start using the G8 Screening Tool calculator, visit: https://oncotoolkit.com/calculator/g8-geriatric-screening. We recommend bookmarking the page on your clinic workstation and mobile device.
At OncoToolkit, we aim to reduce cognitive and administrative burden by turning validated geriatric scores into intuitive calculators. Explore related tools on our platform—such as chemotherapy toxicity risk models (CARG)—to build a cohesive approach to caring for older patients with cancer. [18], [1], [3]
Ready to Optimize Geriatric Screening?
Flag vulnerable patients in seconds and ensure they receive the right assessment before treatment begins.
Use the G8 Calculator Now
Free to use. No registration required.
References
- SIOG Task Force. Geriatric screening tools in cancer patients. Source
- Soubeyran P, et al. Validation of G8 screening tool in ONCODAGE. J Clin Oncol. Source
- OncoToolkit Platform. Source
- Kenis C, et al. Prognostic value of G8 in older cancer patients. PMC. Source
- Evidencio G8 Model details. Source
- eviQ. Geriatric G8 Screening Tool. Source
- SIOG Recommendations Update. PMC. Source
- Lund CM, et al. G8 and survival in lung cancer. PMC. Source
- Bellera CA, et al. Screening with G8 in ONCODAGE project. PMC. Source
- Oncology Nurse Advisor. Optimal strategies for G8 and CGA. Source
- ScienceDirect. Validation of Chinese version G8. Source
- ASCO GOLDEN Study. Asian G8 cut-off validation. Source
- PMC. G8 in urothelial carcinoma treated with IO. Source
- PubMed. G8 and survival in lung cancer immunotherapy. Source
- ASCO Publications. Screening adults 65+ for CGA. Source
- PubMed. G8 and surgical risk stratification. Source
- PMC. Optimized 6-item G8 tool. Source
- CARG Toxicity Risk Models. Sage Journals. Source