CARG Toxicity Score (Geriatric) Calculator: Guideline-Aligned Decision Support for Supportive Care Oncologists
Estimate grade 3–5 chemotherapy toxicity risk in older adults using the evidence-based CARG model, aligned with ASCO and NCCN geriatric oncology guidelines.

Quick Navigation
- 1. Introduction: The Need for CARG Toxicity Scoring
- 2. What is the CARG Toxicity Score (Geriatric)?
- 3. Why the CARG Toxicity Score Matters in Practice
- 4. Clinical Evidence and Validation
- 5. How Our CARG Toxicity Score Calculator Works
- 6. Specific Use Cases and Applications in Clinical Practice
- 7. How the Platform Supports Care, Education, and Research
- 8. Exploratory Modifications and Updates to the CARG Model
- 9. Frequently Asked Clinical Questions
- 10. Conclusion: Use the CARG Toxicity Score Calculator
1. Introduction: The Need for CARG Toxicity Scoring
CARG Toxicity Score (Geriatric) calculator – guideline-aligned chemotoxicity risk tool
Stratify the observed incidence of grade 3–5 chemotherapy toxicity in adults aged 65 years or older who are starting a new cytotoxic chemotherapy regimen. Use the result alongside comprehensive geriatric assessment and clinical judgment.1, 2
Older adults now represent the majority of patients receiving systemic anticancer therapy, and they experience disproportionately high rates of chemotherapy-related toxicity, unplanned hospitalizations, and early treatment discontinuation. Traditional tools such as ECOG performance status and chronological age alone perform poorly in predicting which older adults will experience severe (grade 3–5) chemotherapy toxicity.2, 4, 5, 6
The Cancer and Aging Research Group (CARG) Toxicity Score offers a structured, evidence-based method to estimate the risk of severe chemotherapy toxicity in older adults (commonly ≥65 years) starting a new cytotoxic regimen. At OncoToolkit, we have built a CARG Toxicity Score (Geriatric) calculator specifically for supportive care and emergencies oncologists, translating the original 11‑variable model into a fast, mobile-responsive tool that reduces cognitive load and “calculator fatigue” while remaining consistent with recommendations from the American Society of Clinical Oncology (ASCO), the International Society of Geriatric Oncology (SIOG), and the National Comprehensive Cancer Network (NCCN).3, 5, 7, 1, 2
Our online calculator is available at: /calculator/carg-chemotherapy-toxicity-geriatric-assessment.
2. What is the CARG Toxicity Score (Geriatric)?
The CARG Toxicity Score is a geriatric oncology risk-stratification model for at least one grade 3–5 chemotherapy-related toxicity during treatment. It was derived from a prospective multicenter cohort of 500 adults aged 65 years or older with solid tumors starting a new cytotoxic chemotherapy regimen.7, 1
2.1 Components of the score
The final CARG model assigns 0–3 points to each of 11 pre‑treatment variables, capturing tumor type, regimen intensity, laboratory values, and geriatric assessment (GA)–derived vulnerabilities. Variables and their contributions include:8, 7
- Age ≥72 years (2 points)
- GI or GU cancer type (2 points)
- Planned standard-dose vs reduced-dose chemotherapy (2 points for standard dose)
- Polychemotherapy vs monotherapy (2 points for multi‑agent therapy)
- Hemoglobin below sex-specific thresholds (3 points)
- Jelliffe creatinine clearance using ideal weight <34 mL/min (3 points)
- Hearing impairment rated fair, poor, or deaf (2 points)
- At least one fall in the previous six months (3 points)
- Health limits walking one block somewhat or a lot (2 points)
- Need for assistance taking medications (1 point)
- Decreased social activity due to health (1 point)1, 7
The source weights allow a theoretical total from 0 to 23. Scores observed in the 2011 derivation cohort reached 19, while current ASCO/CARG materials classify 10–23 as high.1, 21
2.2 Risk categories and predicted toxicity
The model stratifies patients into three groups. The percentages below are observed 2011 derivation-cohort incidences of grade 3–5 toxicity, not individualized probabilities:
| Risk group | Score range | 2011 derivation-cohort incidence |
|---|---|---|
| Low risk | 0–5 | 30% |
| Intermediate risk | 6–9 | 52% |
| High risk | 10–23 | 83% |
In the separate 2016 external-validation cohort, observed grade 3–5 toxicity was 36.7%, 62.4%, and 70.2% across the same low, intermediate, and high groups. These are validation-cohort observations, not a second scoring model.21
3. Why the CARG Toxicity Score Matters in Practice
3.1 Integration into geriatric oncology guidelines
ASCO’s geriatric oncology guideline (2018) and its 2023 update recommend that older adults being considered for systemic cancer therapy undergo a geriatric assessment to uncover vulnerabilities not captured by routine oncology evaluation. These guidelines specifically highlight the CARG Toxicity Score and CRASH score as validated instruments that can help predict chemotherapy toxicity and inform decision-making.13, 14, 15, 2
NCCN’s Older Adult Oncology guidelines similarly emphasize integrating GA with validated risk tools, explicitly citing CARG as a model that can be used to estimate chemotherapy-related toxicity and tailor treatment intensity. SIOG consensus statements reinforce the role of GA-based predictive models, including CARG, in guiding systemic therapy decisions in seniors.5, 6, 3
In short, contemporary guidelines encourage using CARG as part of a structured GA process, not as a stand‑alone gatekeeper, and our OncoToolkit calculator is designed to facilitate exactly this pattern of use.2, 3, 5
3.2 Clinical implications for supportive care & emergencies oncologists
For clinicians working in supportive care and emergency oncology settings, the CARG Toxicity Score has several critical applications:
- Prechemotherapy risk discussion
- Risk communication and shared decision-making
- Supportive care resource allocation
Without digital support, using CARG requires recalling 11 weighted variables, performing manual arithmetic, and mapping totals to cohort-incidence groups. The calculator automates those steps while showing the underlying additive trace.1
4. Clinical Evidence and Validation
4.1 Derivation cohort and core performance
The seminal Hurria et al. study included 500 patients aged ≥65 years with solid tumors starting a new chemotherapy regimen across multiple US centers. Key features:7, 1
- Primary endpoint: occurrence of at least one grade 3–5 chemotherapy-related toxicity (CTCAE v3) over the course of treatment.1
- Candidate predictors: demographic variables, tumor type, treatment characteristics, labs, and GA elements.1
- Modeling approach: logistic regression with backward selection to derive the 11-variable CARG model, followed by internal validation.1
- Performance: c‑statistic ~0.72 in the derivation dataset, with clear separation of toxicity rates—30%, 52%, and 83%—across low-, intermediate-, and high-risk groups.7, 1
4.2 External validation and comparative studies
The 2016 external validation enrolled 250 adults aged 65 years or older with solid tumors starting a new chemotherapy regimen. Grade 3–5 toxicity occurred in 36.7% of the low group, 62.4% of the intermediate group, and 70.2% of the high group; these values are reported separately from the derivation incidences and do not alter the additive score.21
Multiple studies have externally validated and extended the CARG model:
- Curative-intent chemotherapy (ELCAPA prospective cohort): Older adults receiving curative-intent chemotherapy for various solid tumors showed progressively higher toxicity rates across CARG risk groups, confirming the original gradients.9
- European and Asian cohorts: Prospective cohorts such as ELCAPA and regional studies in Asia have demonstrated that CARG retains risk discrimination in non‑US populations, although c‑statistics are often in the 0.60–0.65 range.11, 12, 4
- Comparison with CRASH and other instruments: Prospective comparisons between CARG and CRASH indicate that both predict toxicity, with CARG often favored for practicality and ease of implementation.18, 6
- Real-world implementation and outcomes: Observational cohorts and registry analyses generally confirm higher adverse event rates in high-score patients.19, 16, 4
ASCO and NCCN guidelines reference this body of evidence when recommending CARG as a validated tool for integration into GA-based care pathways.3, 14, 2
4.3 Limitations and caveats
Consistent with guideline commentary and the literature:
- The calculator is scoped to adults aged 65 years or older with solid tumors who are starting a new cytotoxic chemotherapy regimen.1, 21
- Predictive performance can vary; CARG should complement—not replace—clinical judgment.12, 11, 9
- Important domains such as cognition and nutrition should still be assessed separately.5, 2
OncoToolkit’s calculator explicitly states that it is a decision-support instrument rather than a prescriptive algorithm.
5. How Our CARG Toxicity Score Calculator Works
Our implementation mirrors the original CARG model while optimizing usability for busy clinicians.
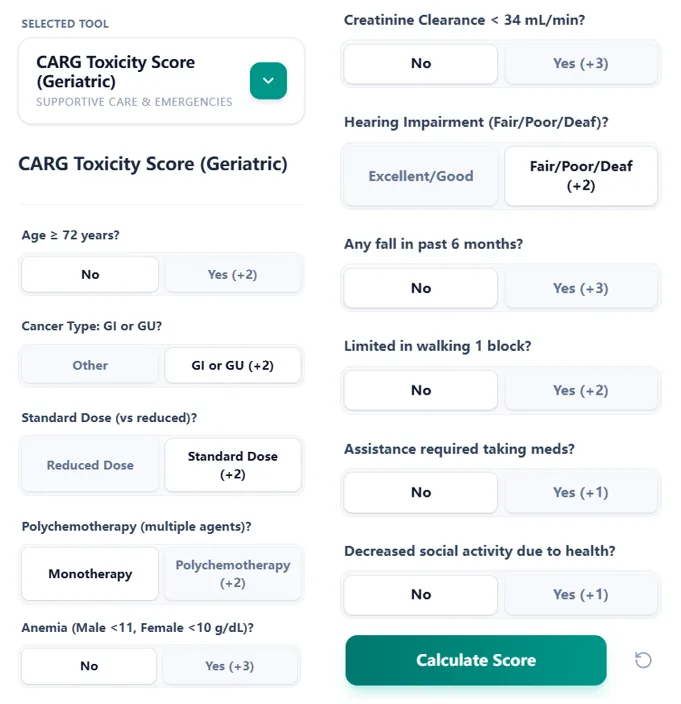
Figure 1. The input interface displays all 11 CARG variables in a single, organized view, enabling rapid data entry during clinic, MDT meetings, or emergency consultations.
Step‑by‑step workflow
- Enter patient and tumor characteristics: Age ≥72 years and GI/GU cancer type are selected via clear yes/no buttons.7
- Specify regimen intensity: Toggling between standard-dose vs reduced-dose and mono vs polychemotherapy automatically applies point values.7
- Add key laboratory and GA factors: Hemoglobin and CrCl thresholds are entered via simple binary options; GA variables are collected through brief, plain-language questions.5, 2, 7
- Calculate and interpret the score: The total maps to a risk group and the corresponding 2011 derivation-cohort incidence, with an additive trace for verification.1
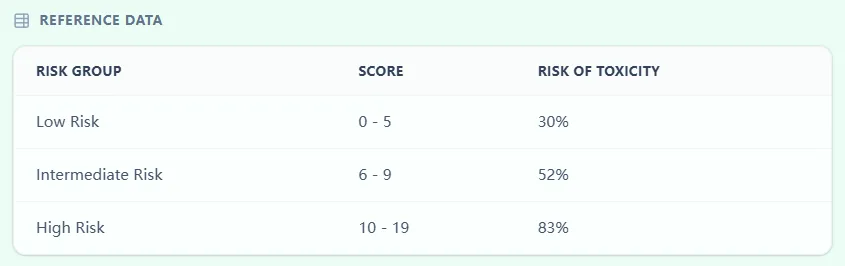
Figure 2. The embedded reference table links score ranges to risk groups, reinforcing categorical interpretation.
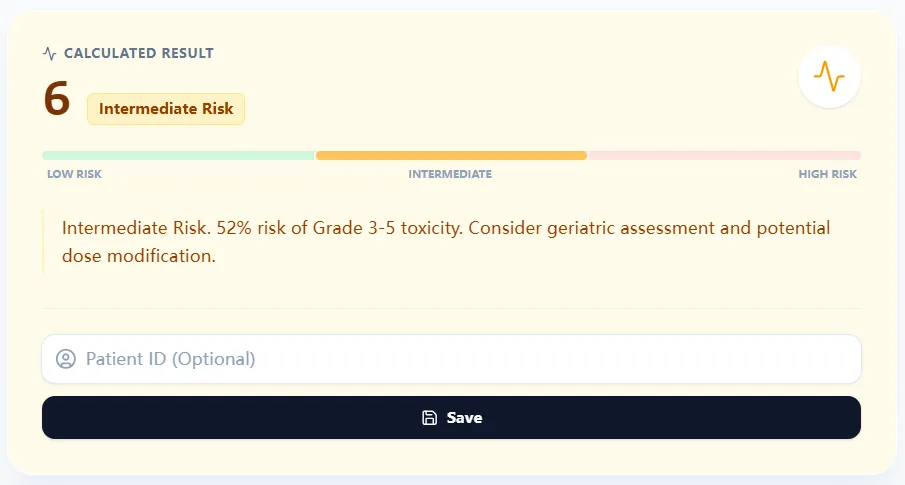
Figure 3. Sample result page showing score 6 and the intermediate group's 52% derivation-cohort incidence of grade 3–5 toxicity.
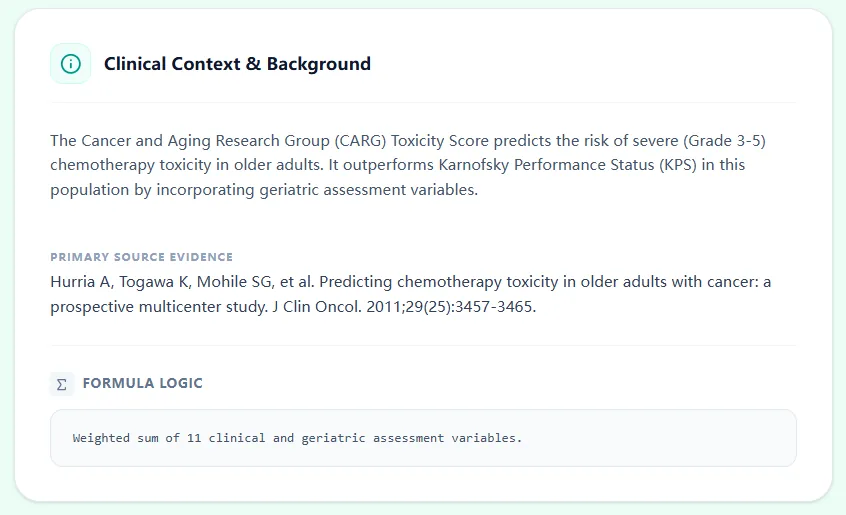
Figure 4. The clinical context panel summarizes the evidence base and reminds users that the tool complements clinical judgment.
6. Specific Use Cases and Applications in Clinical Practice
6.1 Adjuvant chemotherapy in older adults
In an 80‑year‑old with resected stage III colon cancer being considered for adjuvant FOLFOX, supportive care oncologists can:
- Use the CARG calculator to quantify risk based on tumor type, regimen intensity, and GA findings.11, 9
- Discuss the cohort-incidence group alongside the complete geriatric assessment, treatment goals, and clinical context.
- Document the 11 inputs and the role of clinical judgment without treating the score as a prescriptive algorithm.
6.2 First‑line palliative chemotherapy in frail older adults
For a 78‑year‑old with metastatic lung cancer and limited mobility, a high CARG score highlights substantial risk even if ECOG performance appears acceptable, aligning with recommendations for shared decision-making.5, 9, 2
6.4 Multidisciplinary meetings and tumor boards
Standardized CARG scores provide a shared quantitative language for oncologists, geriatricians, and pharmacists to operationalize NCCN and ASCO risk stratification recommendations.9, 2
6.5 Integration with geriatric oncology services
High scores in specialized clinics may prompt prehabilitation interventions (physical therapy, medication optimization) before systemic therapy begins.16, 5
7. How the Platform Supports Care, Education, and Research
7.1 Routine decision support aligned with guidelines
By automating the score, our calculator makes ASCO recommendations feasible in real-world infusion centers and MDT meetings via a mobile-responsive interface.14, 2
7.2 Teaching and trainee development
The calculator serves as a prompt for trainees to discuss why specific factors—like CrCl or social activity—predict toxicity, reinforcing core GA concepts.6, 5
7.3 Clinical research and QI
Institutions can use the tool for local validation or QI projects aimed at reducing unplanned admissions, consistent with priorities in geriatric oncology guidelines.12, 16, 4
8. Exploratory Modifications and Updates to the CARG Model
While the original model remains the standard, exploratory research continues in EHR automation, expanded endpoints (early mortality), and regional recalibrations for specific populations.20, 17, 11
9. Frequently Asked Clinical Questions
ASCO recommends performing a GA for older adults starting systemic therapy. CARG should be layered on top: GA identifies specific vulnerabilities, while CARG quantifies toxicity risk to help prioritize interventions like dose modifications.15, 14, 2
The 30%, 52%, and 83% values are observed incidences in the 2011 derivation cohort. They are not individualized probabilities; the 2016 external-validation observations are reported separately.1, 21
10. Conclusion: Use the CARG Toxicity Score Calculator
The CARG Toxicity Score (Geriatric) is one of the most thoroughly studied and guideline-recognized tools for predicting chemotherapy toxicity in older adults. By embedding the original 11‑variable model into a streamlined, transparent calculator, OncoToolkit enables supportive care and emergency oncologists to apply this evidence at the point of care, consistent with ASCO, SIOG, and NCCN recommendations on GA and risk stratification.2, 3, 4, 5, 1
Ready to Simplify Your Chemotoxicity Risk Assessment?
Calculate the CARG Toxicity Score in seconds and align your treatment plans with global geriatric oncology guidelines.
Use the Calculator Now
Free to use. No registration required.
References
- Hurria A, et al. Predicting Chemotherapy Toxicity in Older Adults with Cancer: A Prospective Multicenter Study. Source
- Mohile SG, et al. Practical Assessment and Management of Vulnerabilities in Older Patients Receiving Chemotherapy: ASCO Guideline for Geriatric Oncology. Source
- NCCN Clinical Practice Guidelines in Oncology: Older Adult Oncology. Source
- Loh KP, et al. Geriatric Assessment-Guided Interventions in Older Adults with Cancer. Source
- Wildiers H, et al. International Society of Geriatric Oncology Consensus on Geriatric Assessment in Older Patients with Cancer. Source
- Extermann M, et al. Comparison of Different Tools for Predicting Chemotherapy Toxicity in Older Patients. Source
- Hurria A, et al. Development of a Prediction Model for Chemotherapy Toxicity in Older Adults. Source
- A Simple Tool for Predicting Chemotherapy Toxicity in Older Adults. Source
- Curative-Intent Chemotherapy and Toxicity Risk in Older Adults. Source
- Score Range and Toxicity Probability in Older Adults. Source
- External Validation of the CARG Score in European Cohorts. Source
- Validation of the CARG Score in Asian Populations. Source
- ASCO Geriatric Oncology Guideline Update 2023. Source
- Geriatric Assessment-Driven Care Pathways. Source
- ASCO 2023 Geriatric Assessment Update Slides. Source
- Implementation of Geriatric Oncology Guidelines in Clinical Practice. Source
- CARG Score and Emergency Department Visits. Source
- Comparative Performance of CARG and CRASH Scores. Source
- Retrospective Single-Center Study on CARG Score Performance. Source
- EHR-Derived Toxicity Risk Prediction Models. Source
- Hurria A, et al. Validation of a Prediction Tool for Chemotherapy Toxicity in Older Adults With Cancer. Source