SINS (Spinal Instability) Calculator: The Definitive Clinical Guide to Tumor-Related Spinal Instability Assessment
Assess spinal stability in neoplastic disease with the SINS calculator on OncoToolkit. Get instant stability classification and surgical referral guidance — try it now.

Quick Navigation
- 1 Introduction: The Challenge of Spinal Metastases
- 2 What Is the Spinal Instability Neoplastic Score (SINS)?
- 2 1 The Six Components of SINS
- 3 Why SINS Matters in Daily Spine Oncology Practice
- 4 How SINS Fits Within Broader Decision Frameworks
- 5 Clinical Evidence and Validation
- 6 How Our SINS Calculator Works
- 7 Supporting Clinical Care, Education, and Research
- 8 Clinical FAQ
- 9 Special Populations: Use With Caution
- 10 Start Using the SINS Calculator Today
1 Introduction: The Challenge of Spinal Metastases
Spinal metastases affect up to 40% of patients with advanced cancer, and distinguishing mechanical instability from simple painful disease is one of the most nuanced decisions in musculoskeletal oncology. The consequences of getting it wrong are significant: under-recognition of instability risks progressive deformity, pathologic fracture, and neurologic deterioration, while over-referral burdens surgical teams and delays radiation therapy. For years, physicians relied on experience and informal criteria — an approach that was neither reproducible nor easily communicated across disciplines 1, 2, 3, 4.
The Spinal Instability Neoplastic Score (SINS) was developed by the Spine Oncology Study Group (SOSG) specifically to solve this problem. It translates six clinical and radiographic parameters into a single numeric score (0–18) that stratifies lesions as stable, indeterminate, or unstable. At OncoToolkit, we've built a dedicated SINS (Spinal Instability) calculator that lets you complete this assessment in under a minute — on any device, during an MDT meeting, at the bedside, or in clinic. You can access it here: /calculator/sins-spinal-instability-neoplastic-score 3, 5, 6, 7.
This article walks through the clinical rationale behind SINS, the evidence supporting its use, and exactly how to use our calculator to improve consistency, speed, and quality of care for patients with neoplastic spine disease.
2 What Is the Spinal Instability Neoplastic Score (SINS)?
The SINS is a semi-quantitative classification system introduced by Fisher and colleagues in 2010, developed through a systematic literature review and a modified Delphi consensus process among international spine oncology experts. The SOSG defined neoplastic spinal instability as "loss of spinal integrity as a result of a neoplastic process that is associated with movement-related pain, symptomatic or progressive deformity, and/or neural compromise under physiologic loads" 2, 8, 7, 3.
Before SINS, clinicians applied trauma- or degenerative-based instability models to tumor patients, which was problematic because pathologic fractures do not behave like traumatic fractures — ligaments and discs are less commonly affected by tumors, and the capacity for bone healing is compromised. SINS was the first system to integrate tumor-specific biomechanics into a validated, reproducible scoring framework 4, 2, 3.
2 1 The Six Components of SINS
The SINS total (range 0–18) is the arithmetic sum of six individually scored parameters — one clinical and five radiographic 5, 6, 9:
| Component | Options | Points |
|---|---|---|
| Location | Junctional (occiput–C2, C7–T2, T11–L1, L5–S1) | 3 2 1 0 |
| Pain | Mechanical (improves with recumbency; worsens with movement/loading) | 3 1 0 |
| Bone Lesion Quality | Lytic Mixed (lytic/blastic) Blastic | 2 1 0 |
| Radiographic Spinal Alignment | Subluxation / translation De novo deformity (kyphosis/scoliosis) Normal alignment | 4 2 0 |
| Vertebral Body Collapse | >50% collapse | 3 2 1 0 |
| Posterolateral Involvement | Bilateral Unilateral None | 3 1 0 |
Each component was weighted through expert consensus based on its perceived contribution to spinal biomechanical integrity in the setting of tumor. The alignment component carries the greatest single-item weight (up to 4 points), reflecting the high clinical significance of translational deformity 6, 3, 5.
3 Why SINS Matters in Daily Spine Oncology Practice
3 1 Standardized Language Across Disciplines
One of the most powerful features of SINS is that it provides a shared, reproducible vocabulary for instability. An orthopedic oncologist, a radiation oncologist, and a radiologist can each calculate the score independently and arrive at a consistent triage decision. Validation studies have confirmed substantial to excellent inter-observer reliability (intraclass correlation coefficient 0.846 for total score) and near-perfect reliability when scores are collapsed into the three clinical categories 10, 8, 11, 12, 4.
3 2 Guiding Surgical Referrals
The three SINS categories map directly to clinical action 4, 6:
- 0–6 (Stable): Typically managed with radiation therapy, systemic therapy, or observation. Surgical referral is not routinely required for instability alone.
- 7–12 (Indeterminate / Impending Instability): Surgical consultation is recommended to further evaluate stability and determine if fixation, cement augmentation, or additional imaging is needed.
- 13–18 (Unstable): Surgical stabilization is generally indicated; these patients should be referred to a spine surgeon before radiation or other interventions proceed.
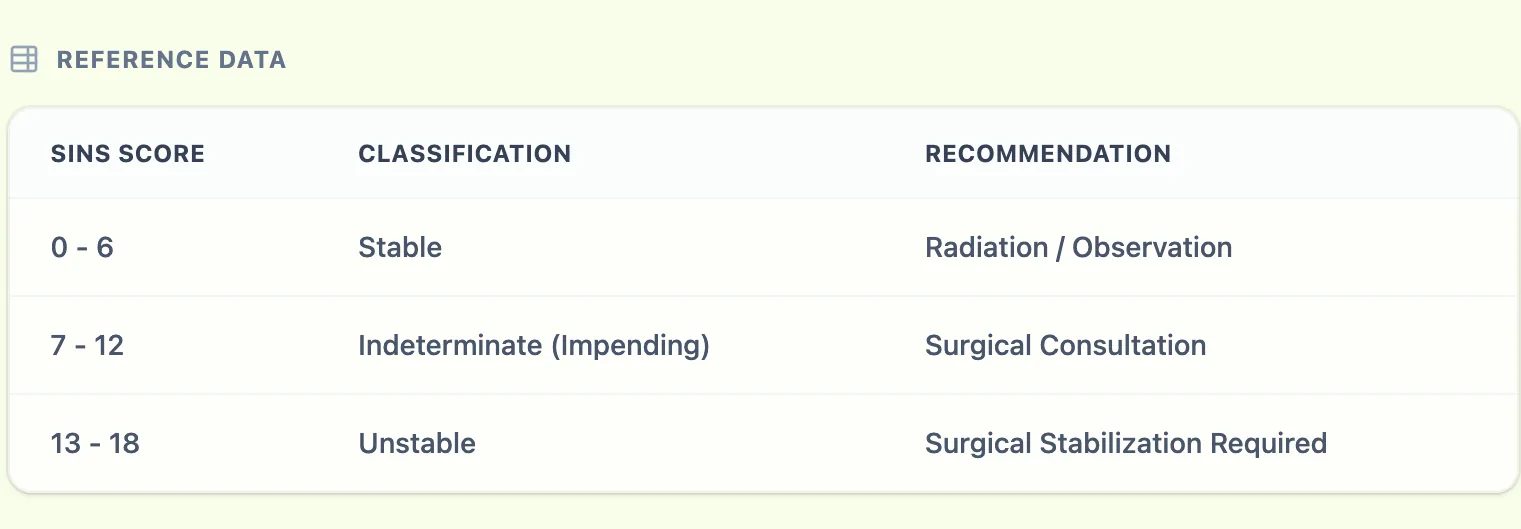
Figure 1. The SINS reference table on OncoToolkit maps total scores to stability categories.
3 3 Reducing Calculator Fatigue at Point of Care
In a busy spine oncology or radiation oncology clinic, scoring six discrete components quickly becomes a source of cognitive load. Mental arithmetic errors are common when clinicians are toggling between imaging and records. Our platform is mobile-responsive and designed for rapid one-tap-per-component input, eliminating the need to remember point values 1, 4.
4 How SINS Fits Within Broader Decision Frameworks
4 1 SINS and the NOMS Framework
SINS does not function in isolation. At many high-volume spine metastasis centers, it is integrated into the NOMS (Neurologic, Oncologic, Mechanical, Systemic) framework. Within NOMS, SINS provides the structured assessment for the "M" (Mechanical) domain 13, 14, 15, 1.
The NOMS algorithm proceeds through four sequential checkpoints 1:
- Neurologic: Degree of epidural spinal cord compression (ESCC grade).
- Oncologic: Radiosensitivity of the tumor histology.
- Mechanical: SINS-based stability assessment.
- Systemic: Overall disease burden, prognosis, fitness for surgery.
Pearl: By pairing the SINS calculator with other tools on OncoToolkit—such as the ECOG Performance Status or the Charlson Comorbidity Index—clinicians can systematically work through the NOMS algorithm digitally.
4 2 When Should You Not Rely Solely on SINS?
SINS assesses biomechanical instability; it was not designed to evaluate the severity of epidural cord compression, tumor histology, or systemic prognosis. A spine with a low SINS (e.g., 4) may still require urgent surgery if there is high-grade ESCC from a radioresistant tumor. Conversely, a high SINS (e.g., 15) does not automatically mean a patient is a surgical candidate if performance status precludes safe intervention 14, 3, 4, 1.
5 Clinical Evidence and Validation
5 1 The Math Behind the Tool
The SINS is an additive, point-based system — not a regression model. Each of the six components contributes a discrete integer score derived from expert-consensus weighting, and the total is a simple arithmetic sum (range 0–18). There is no Cox regression coefficient, hazard ratio, or logistic function underlying the final score. This simplicity is deliberate: it ensures that the score can be calculated by any clinician, in any setting, without software — though a dedicated calculator eliminates arithmetic error entirely 3, 5, 6.
The thresholds (0–6, 7–12, 13–18) were determined by the SOSG consensus panel based on clinical face validity, and subsequently validated against expert surgeon opinion as the reference standard 10, 3.
5 2 Reliability Across Specialties
One of the strongest features of SINS is its cross-disciplinary reliability:
- Spine oncology surgeons: Inter-observer ICC of 0.846 (95% CI 0.773–0.911); intra-observer ICC of 0.886 (95% CI 0.868–0.902) 12, 10.
- Radiologists: Excellent validity (κ = 0.88) and substantial inter-observer agreement (κ = 0.76) on the binary scale 8.
- Radiation oncologists: Substantial inter-observer reliability (κ = 0.76) and excellent intra-observer reliability (κ = 0.80) 11.
5 3 Predicting Post-Radiation Vertebral Compression Fractures
Beyond its original purpose of triaging instability, SINS has demonstrated utility in predicting vertebral compression fractures (VCF) following spine stereotactic body radiotherapy (SBRT). A multi-institutional analysis of 410 spinal segments found that higher SINS were significant predictors of post-SBRT fracture. The 1-year cumulative incidence of VCF was approximately 12%, with 65% of fractures occurring within the first four months. This finding has important implications: SINS should be calculated before SBRT to identify patients who may benefit from prophylactic cement augmentation 17, 18.
5 4 Limitations and Caveats
A systematic review of 21 studies found that not all components perform equally. The "location" parameter showed near-perfect inter-observer agreement but no independent accuracy for predicting VCF. The "bone lesion quality" component had significant predictive accuracy in half of the studies but only fair inter-observer reliability. These findings suggest that while the composite score remains robust, individual component interpretation requires careful imaging review — ideally with CT rather than MRI alone 19, 20, 12.
Figure 2. The OncoToolkit SINS calculator reinforces transparency and methodology at point of care.
6 How Our SINS Calculator Works
At OncoToolkit, the SINS (Spinal Instability) calculator is built to mirror the original Fisher et al. scoring system exactly, with no modifications to component definitions or point values 5, 3.
6 1 Step 1: Enter the Six Parameters
Open the calculator at /calculator/sins-spinal-instability-neoplastic-score. You will see six dropdown fields 5:
- Location — Select the spinal region (Junctional, Mobile, Semirigid, or Rigid).
- Pain Relief with Recumbency (Mechanical Pain) — Indicate mechanical pain, occasional non-mechanical pain, or pain-free.
- Bone Lesion Quality — Choose lytic, mixed, or blastic.
- Radiographic Spinal Alignment — Select subluxation/translation, de novo deformity, or normal alignment.
- Vertebral Body Collapse — Indicate the degree of collapse or body involvement.
- Posterolateral Involvement (Facets/Pedicles) — Select bilateral, unilateral, or none.
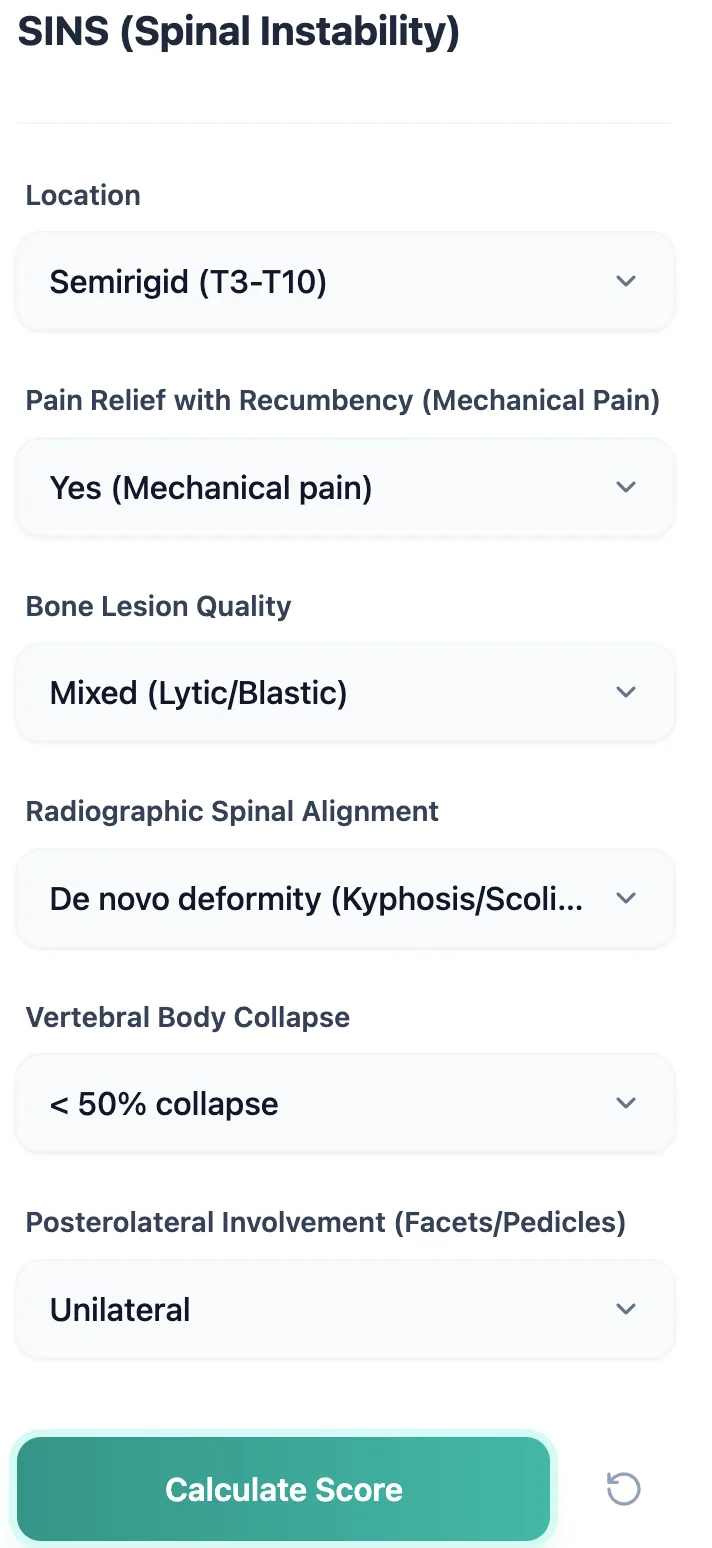
Figure 3. The SINS input form displays all six scoring parameters as dropdown menus with clear labels.
6 2 Step 2: Calculate and Interpret the Result
Tap "Calculate Score" and the tool instantly returns:
- The total SINS numeric value.
- The stability classification (Stable, Indeterminate / Impending Instability, or Unstable).
- A visual risk bar showing where the score falls on the spectrum.
- A plain-language recommendation (e.g., "Surgical consultation recommended").
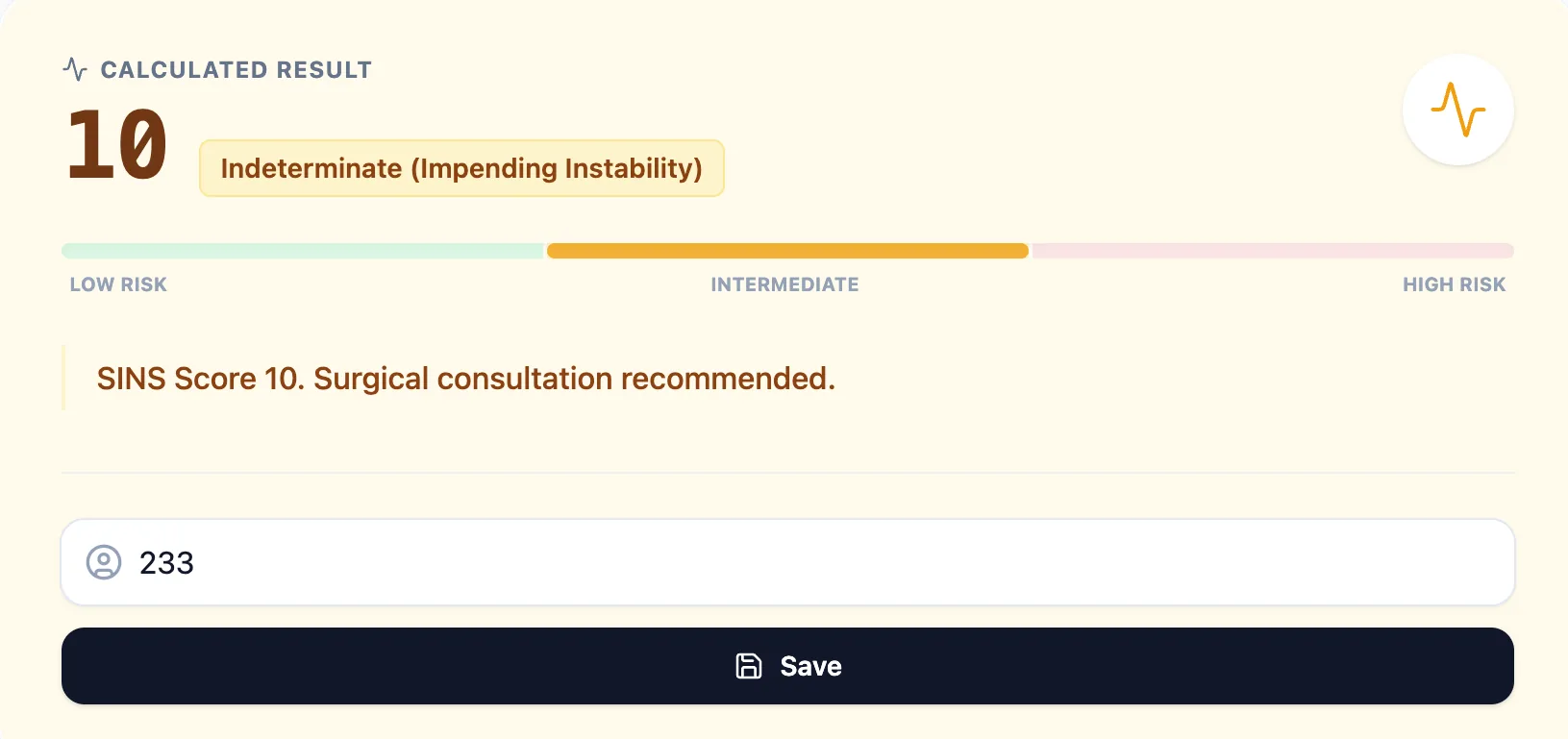
Figure 4. The result screen for a SINS score of 10 — classified as Indeterminate (Impending Instability).
6 3 Step 3: Save and Export
Results can be saved directly within the platform and exported for documentation in clinical notes, MDT records, or research databases 21.
7 Supporting Clinical Care, Education, and Research
In daily practice, the SINS calculator is most valuable at initial staging and during MDT preparation. For spine oncology fellows and residents, it serves as a teaching tool. Using SINS consistently across a cohort enables reliable stratification for research and quality improvement protocols 6, 1, 14.
8 Clinical FAQ
Can the SINS Be Used for Primary Spinal Tumors?
Yes. Although originally developed for metastases, it assesses biomechanical instability caused by any neoplastic process. However, reconstruction considerations for primary tumors differ 23, 3.
9 Special Populations: Use With Caution
Clinicians should exercise additional judgment in:
- Pediatric patients: SINS was validated in adults.
- Prior spinal instrumentation: Hardware may mask radiographic parameters.
- High-grade spinal deformity unrelated to tumor: Should be distinguished from de novo deformity.
- Purely epidural disease: Better captured by ESCC grading within NOMS 2, 1.
10 Start Using the SINS Calculator Today
- Open the calculator at /calculator/sins-spinal-instability-neoplastic-score.
- Try it with cases you have seen recently.
- Bookmark it for instant access during rounds.
- Save and export results for consistent documentation.
Ready to Simplify Your Spinal Stability Assessments?
Access our mobile-optimized SINS calculator for instant scoring and surgical referral guidance.
Try the SINS Calculator
Free to use. No registration required.
Disclaimer: This calculator is a clinical decision-support tool based on the published Spinal Instability Neoplastic Score (Fisher et al., 2010). It does not replace the clinical judgment of a qualified physician. All treatment decisions should be made in the context of the individual patient's clinical presentation and institutional protocols.
References
- Laufer et al. The NOMS Framework for decision making in spine metastases. Source
- Neoplastic Spinal Instability: Pathophysiology and Assessment. Source
- DukeSpace: Clinical analysis of SINS reliability. Source
- SINS Reliability and Validity Study. Source
- CancerCalc: SINS Calculation logic. Source
- PACS: Terminology for SINS. Source
- Fisher et al. SOSG Consensus Statement on SINS. Source
- AJR: Radiologist Validation of the SINS System. Source
- Oxford Med Ed: Scoring Systems in MSCC. Source
- JCO: Reliability Study from the SOSG. Source
- Radiation Oncology Validation of SINS Categories. Source
- URMC Ortho: Analysis of Reliability and Validity. Source
- WUSTL: Decision Making Algorithms for Spine Metastases. Source
- WUSTL Profiles: NOMS Sequential Checkpoints. Source
- MSKCC NOMS Mechanical Domain. Source
- OncoToolkit Resource Hub. Source
- MD Anderson: VCF after SBRT Study. Source
- JCO: Predicting Post-SBRT Fracture Risk. Source
- Systematic Review of 21 SINS validation studies. Source
- SNUCM: Predictive Accuracy of SINS Components. Source
- OncoToolkit Analytics and Survival Dashboards. Source
- MDApp: Clinical Context of SINS Application. Source