Febrile Neutropenia Triage: MASCC and CISNE Risk Scoring
Master Febrile Neutropenia triage using MASCC and CISNE scores. Optimize risk stratification and clinical decision-making for oncologic emergencies.

Quick Navigation
- Introduction to Febrile Neutropenia Triage
- What is Febrile Neutropenia and Why Risk Stratification Matters
- The MASCC Risk Index: Validated Foundation for Low-Risk Identification
- The CISNE Score: Precision Risk Stratification for Stable Patients
- How Our Unified Calculator Works: Streamlining Clinical Workflow
- The Math Behind the Tool: Score Development and Validation
- Clinical Evidence: Validation Studies and Outcomes Data
- Platform Support for Care, Education, and Research
- Limitations and Contraindications
- Frequently Asked Questions (FAQ)
1. Introduction to Febrile Neutropenia Triage
Febrile neutropenia (FN) represents one of the most urgent oncologic emergencies, occurring in 5–10% of patients with solid tumors and up to 85–95% of those with hematologic malignancies receiving chemotherapy. With mortality rates ranging from 2.6% to 9.5% and average hospitalization costs exceeding $40,000 per episode, accurate risk stratification at the point of care is not just clinically important—it's potentially life-saving. Yet clinicians face a persistent challenge: traditional risk assessment tools often rely on subjective criteria, generate inconsistent results across different patient populations, and contribute to "calculator fatigue" during high-pressure clinical decision-making [1], [2], [3], [4], [5].
At OncoToolkit, we've built a unified Febrile Neutropenia Triage calculator that integrates both the MASCC Risk Index and the CISNE score into a single, mobile-responsive platform. This combined approach leverages the strengths of each scoring system—MASCC's high sensitivity for detecting low-risk patients and CISNE's superior specificity for stable-appearing solid tumor patients—to support evidence-based triage decisions in emergency departments, multidisciplinary tumor board meetings, and teaching rounds [6], [7], [8].
2. What is Febrile Neutropenia and Why Risk Stratification Matters
Febrile neutropenia is defined as a single oral temperature ≥38.3°C (or ≥38.0°C sustained over one hour) in a patient with an absolute neutrophil count < 500 cells/µL or < 1,000 cells/µL with expected decline to < 500 within 48 hours. The condition places patients at immediate risk for life-threatening infections: approximately 20–30% have identifiable infection sources, 10–25% develop bacteremia, and 25–30% experience severe complications including septic shock, respiratory failure, or acute kidney injury [2], [9], [10], [1].
Clinical Pearl: While gram-positive organisms now predominate due to fluoroquinolone prophylaxis, gram-negative bacteria—particularly E. coli, K. pneumoniae, and P. aeruginosa—remain responsible for the most severe infections.
3. The MASCC Risk Index: Validated Foundation for Low-Risk Identification
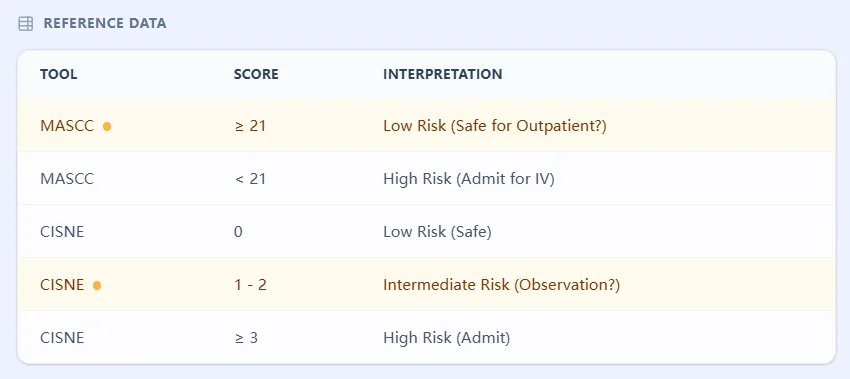
The Multinational Association for Supportive Care in Cancer (MASCC) Risk Index, developed in 2000, emerged from a prospective multinational study designed to identify independent predictors of serious complications. Patients scoring ≥21 are classified as low-risk, with a positive predictive value of 91% for uncomplicated recovery [18], [19], [20], [21], [22].
3.1 MASCC Score Components
- Burden of illness (no/mild symptoms): 5 points
- Absence of hypotension (SBP >90 mmHg): 5 points
- No COPD: 4 points
- Solid tumor/no previous fungal infection: 4 points
- No dehydration requiring IV fluids: 3 points
- Outpatient status: 3 points
- Age < 60 years: 2 points
3.2 Clinical Evidence Supporting MASCC
A 2016 validation study found that MASCC correctly predicted uncomplicated outcomes in 93% of low-risk patients, with no mortality documented in this group. However, in emergency settings, MASCC's sensitivity (78.8%) makes it a powerful tool for ruling out high-risk patients who require immediate intervention [19], [8].
4. The CISNE Score: Precision Risk Stratification for Stable Patients
The Clinical Index of Stable Febrile Neutropenia (CISNE) addresses a critical gap: identifying apparently stable patients who may still develop serious complications [26], [27].
4.1 CISNE Score Components and Mathematical Foundation
- ECOG PS ≥ 2: 2 points
- Stress-induced hyperglycemia: 2 points
- COPD: 1 point
- Chronic cardiovascular disease: 1 point
- Mucositis grade ≥ 2: 1 point
- Monocyte count < 200 cells/µL: 1 point
4.2 Why CISNE Excels in Solid Tumors
In validation cohorts, CISNE achieved an AUC of 0.868, significantly outperforming MASCC's 0.721 in stable solid tumor populations. It specifically identifies the 32% of "stable" patients who might otherwise deteriorate [30], [26].
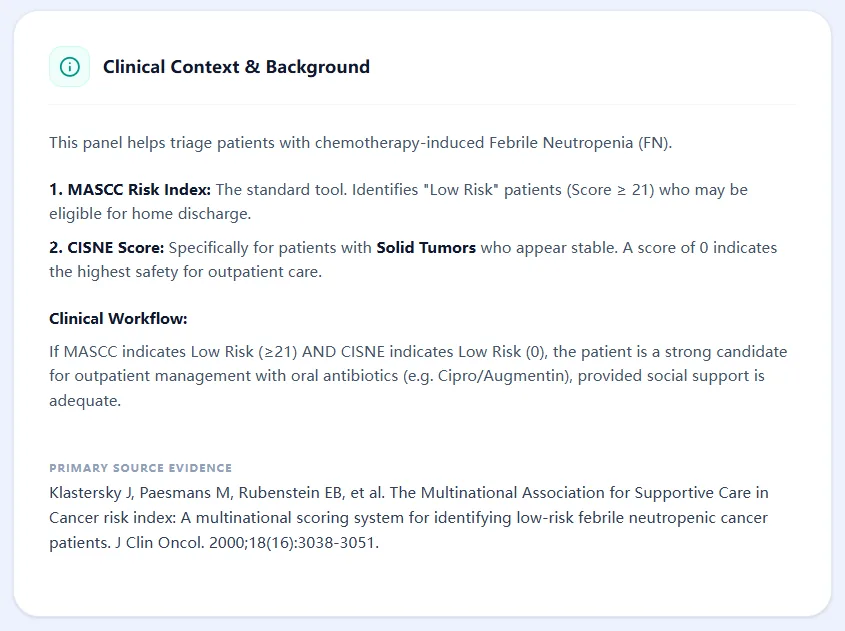
5. How Our Unified Calculator Works: Streamlining Clinical Workflow
5.1 Input Data Collection
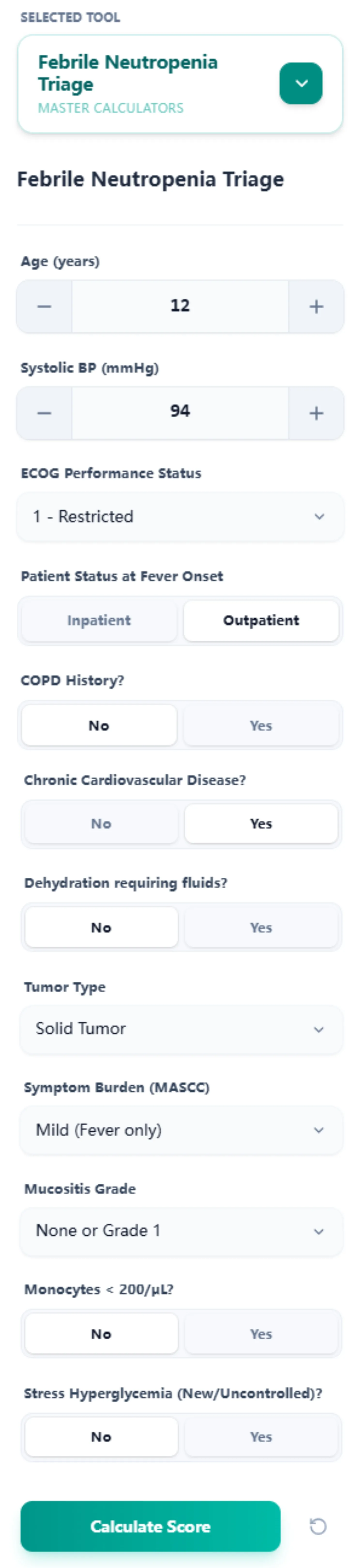
Our calculator consolidates all inputs into a single interface. By capturing age, vital signs, ECOG status, and specific comorbidities, we eliminate redundant data entry.
5.2 Algorithm Logic and Score Interpretation
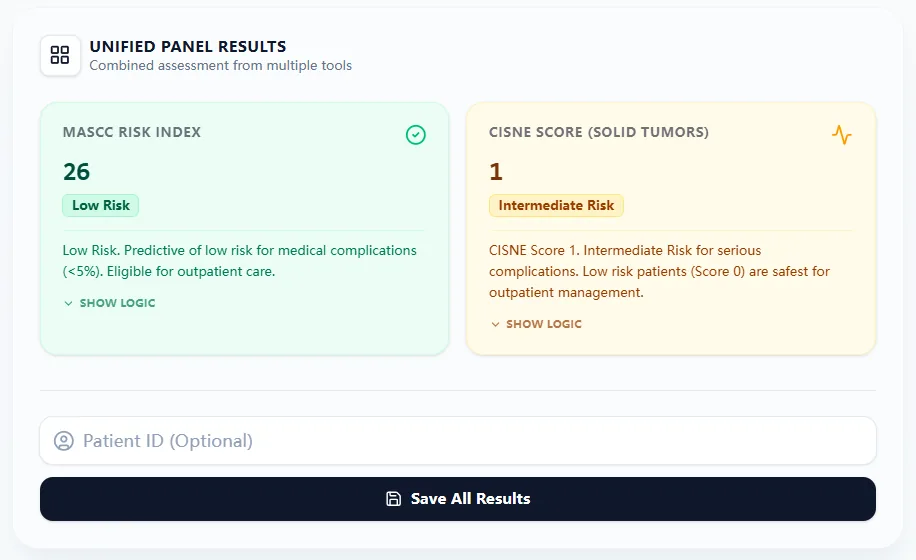
Upon submission, the tool generates a color-coded results panel. MASCC ≥21 (Green) suggests low risk, while CISNE Class 0 indicates the highest safety for outpatient care.
5.3 Transparency and Educational Features
The "Show Logic" functionality ensures the tool isn't a "black box," detailing exactly how each clinical finding contributes to the final score [33], [34].
6. The Math Behind the Tool: Score Development and Validation
6.1 MASCC Development: Multivariate Logistic Regression Model
Developed via multivariate logistic regression on 756 episodes, MASCC was designed to maximize positive predictive value for identifying low-risk recovery candidates [20], [21].
6.2 CISNE Development: Cox Proportional Hazards Analysis
CISNE utilized a Cox proportional hazards model, prioritizing the temporal dimension of risk in stable patients [26].
6.3 Comparative Performance Across Populations
While MASCC is a robust first-line screen, CISNE provides superior specificity in solid tumors (88.2% vs. 75.7%), reducing false-positive high-risk classifications [8], [25].
7. Clinical Evidence: Validation Studies and Outcomes Data
7.1 Impact on Time-to-Antibiotics and Length of Stay
Implementing risk protocols has been shown to reduce time-to-antibiotics from over 200 minutes to under 90 minutes, meeting critical ASCO benchmarks [17], [36].
7.2 Outpatient Management Safety and Efficacy
Low-risk patients (MASCC ≥21) managed with oral ciprofloxacin and amoxicillin-clavulanate have shown a 96% success rate in single-institution series [31].
7.3 Impact on Chemotherapy Dose Intensity
Febrile neutropenia risk scores also correlate with the ability to maintain chemotherapy dose intensity (RDI), which is critical for survival in adjuvant settings [40], [41].
8. Platform Support for Care, Education, and Research
The OncoToolkit platform supports clinical decision-making, residency education through "Show Logic" features, and cohort research via CSV data export [44], [46].
9. Limitations and Contraindications
Warning: Obvious clinical instability (hypotension, organ failure) always overrides calculated risk scores. These patients require immediate hospitalization and IV antibiotics.
Additionally, scores may underestimate risk in patients with acute leukemia undergoing induction or those with recent HSCT [14], [12].
10. Frequently Asked Questions (FAQ)
Can FN patients be safely managed at home?
Yes, if they meet low-risk criteria, have 24/7 caregiver support, and reside within one hour of a facility [11].
What is the most common mistake in calculation?
Subjective assessment of the "burden of illness" in MASCC is the most frequent source of inter-rater variability [5].
Ready to Simplify Your Clinical Triage?
Calculate risk scores in seconds and access validated clinical management guidance immediately.
Access the Febrile Neutropenia Triage Calculator
Free to use. No registration required.
References
- StatPearls: Febrile Neutropenia. Source
- Scientific Reports: MASCC usage in clinics. Source
- Journal of Clinical Oncology: Risk stratification studies. Source
- BMJ Family Medicine: Decision fatigue in oncology. Source
- Nature: Limitations of subjective criteria in MASCC. Source
- Nature: Triage score comparisons. Source
- ScienceDirect: MASCC Meta-analysis. Source
- PubMed: Comparative sensitivity of triage scores. Source
- Nature: Definitions of Febrile Neutropenia. Source
- PMC: Antibiotic benchmarks for FN. Source
- US Pharmacist: Outpatient FN Management. Source
- AJMC: Guidelines in Clinical Practice. Source
- IDSA Guidelines: Clinical practice for FN. Source
- ASH News: Impact of protocols on time-to-antibiotics. Source
- eviQ: Clinical resource for evaluation. Source
- PMC: MASCC Validation in 2016. Source
- JCO: Original MASCC Study (Klastersky). Source
- JCO: Multivariate logic in MASCC. Source
- MDApp: MASCC Calculation breakdown. Source
- Academia: CISNE vs MASCC in Solid Tumors. Source
- JCO: Original CISNE Development Study. Source
- JCO: Validation of the CISNE Score. Source
- MDApp: CISNE risk categories. Source
- CancerCalc: CISNE logic. Source
- JCO: Outpatient success rates. Source
- PMC: The black box problem in CDS. Source
- Nature: Algorithmic aversion in clinicians. Source
- Sacred Heart: DNP Project on time-to-antibiotics. Source
- PubMed: Myelosuppression impact on RDI. Source
- CancerNetwork: Economic impact of neutropenia. Source
- PMC: Diagnostic reasoning in education. Source
- YouTube: Data export tutorial for OncoToolkit. Source