Child-Pugh Score Calculator: Essential Clinical Decision-Making for Cirrhosis Severity and Transplant Prioritization
Rapidly assess cirrhosis severity with our Child-Pugh Score calculator. Stratify transplant urgency, predict survival, and support MDT decisions in seconds.
Quick Navigation
1. Introduction to Child-Pugh Score in Clinical Practice
Cirrhosis management demands rapid, standardized risk assessment at every clinical touchpoint—from initial diagnosis through transplant evaluation to perioperative planning. Yet manually calculating prognostic scores across five variables, while reconciling conflicting classification systems, remains a source of inefficiency and potential error in busy hepatology practices and multidisciplinary tumor boards. The Child-Pugh Score has been the gold standard for stratifying cirrhotic patients into risk categories for over five decades, guiding everything from surgical eligibility to transplant prioritization. However, translating laboratory values into interpretable risk categories without a reliable tool introduces cognitive load and delays clinical decision-making.
At OncoToolkit, we've built an integrated Child-Pugh Score calculator designed specifically for modern hepatology workflows. This tool eliminates manual calculation, surfaces transparent logic for trainees and colleagues, and enables rapid risk stratification at point of care. Whether you're preparing for an MDT meeting, assessing perioperative risk, or teaching fellows about cirrhosis prognosis, our calculator delivers instantaneous, evidence-grounded results—freeing you to focus on clinical judgment rather than arithmetic.
2. What Is the Child-Pugh Score?
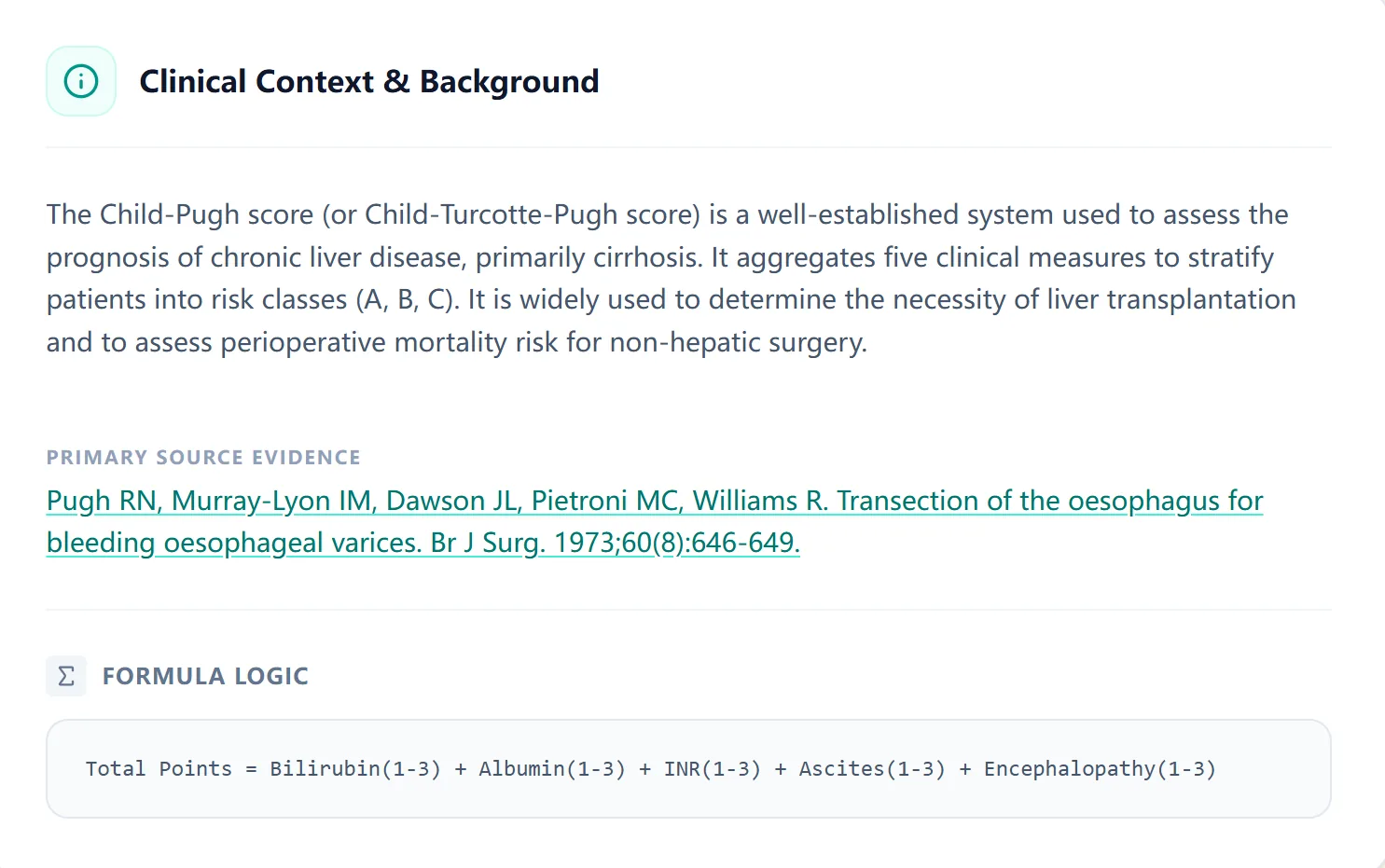
The Child-Pugh Score (also known as the Child-Turcotte-Pugh or CTP score) is a validated, point-based classification system designed to assess the prognosis and severity of chronic liver disease, particularly cirrhosis. Originally developed by Child and Turcotte in 1964 as a tool for selecting surgical candidates for portal decompression, the score was refined by Pugh et al. in 1972 and remains the most widely adopted prognostic framework in hepatology worldwide.
The score aggregates five readily available clinical and laboratory parameters, each contributing 1–3 points based on severity:
- Total bilirubin (1–3 pts)
- Serum albumin (1–3 pts)
- INR or prothrombin time (1–3 pts)
- Ascites (1–3 pts)
- Hepatic encephalopathy (1–3 pts)
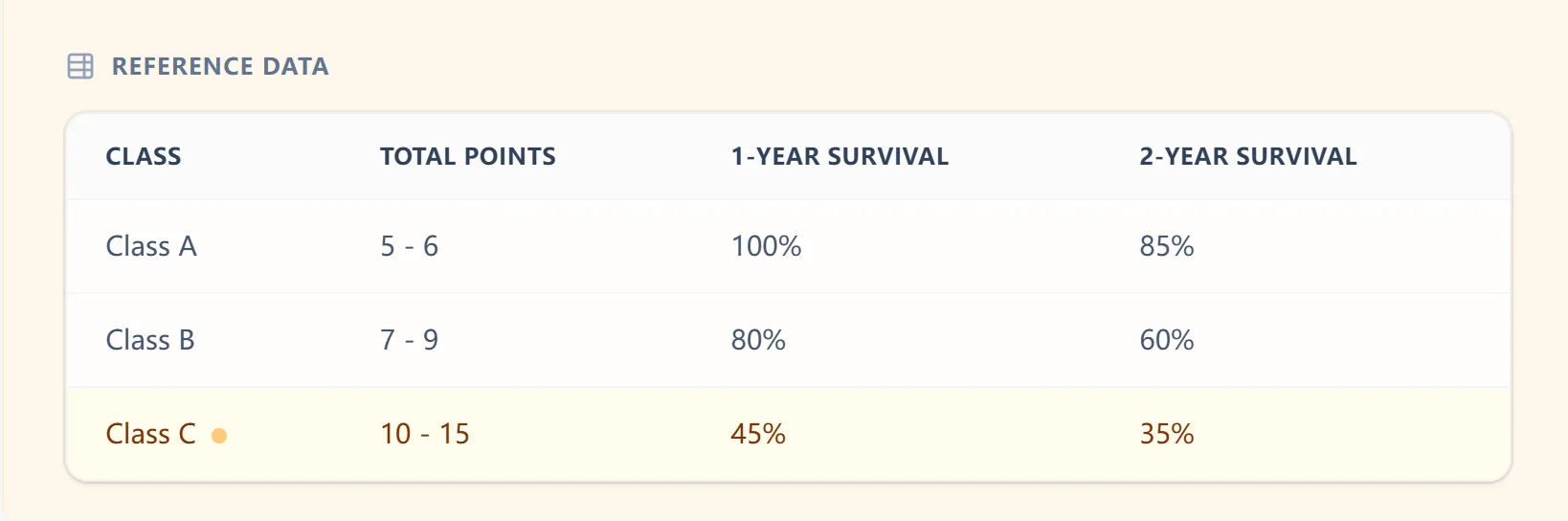
The total score ranges from 5 to 15 points, stratifying patients into three prognostic classes:
3. Why the Child-Pugh Score Matters in Practice
3.1 Clinical Decision-Making Across Multiple Domains
The Child-Pugh Score is far more than a retrospective prognostic marker—it directly informs actionable clinical decisions:
Transplant Listing and Urgency: Class C patients (and some Class B patients with specific complications) are candidates for urgent liver transplant evaluation. The score helps prioritize patients within finite organ allocation systems and informs discussions about bridging therapies.
Perioperative Risk Stratification: Child-Pugh classification predicts mortality during non-hepatic surgery and guides anesthetic and surgical planning. Class C patients face substantially elevated perioperative mortality and require intensive optimization before elective procedures.
Treatment Intensity and Monitoring: Hepatology guidelines embed Child-Pugh classification into management pathways for esophageal varices screening, hepatic encephalopathy prophylaxis, and HCC surveillance intensity. Class C patients warrant more aggressive surveillance and intervention thresholds.
Medication Dosing: Many drug manufacturers recommend dose adjustments based on Child-Pugh class, particularly for renally cleared agents and those metabolized hepatically (antiretrovirals, immunosuppressants, chemotherapy agents).
3.2 The Challenge Without Digital Support
In traditional workflow, calculating Child-Pugh Score requires:
- Identifying or retrieving five separate lab values (some in non-standard units)
- Mentally mapping each value to its point category (e.g., bilirubin 35 µmol/L = 2 points)
- Summing points while cross-checking thresholds
- Referring to a separate reference table to assign class and look up survival statistics
- Documenting the score and its implications in the clinical note
In a hepatology MDT, where 10–20 patients may be discussed, this process consumes precious time and introduces transcription errors. For trainees, the lack of immediate feedback obscures the clinical meaning of each variable's contribution to overall risk.
3.3 How Our Calculator Addresses Real Workflow Constraints
On our platform, this process occurs in seconds. The mobile-responsive interface accepts inputs in multiple units (mg/dL or µmol/L for bilirubin, g/dL or g/L for albumin), automatically maps each to its point value, and displays:
- Instantaneous total score and class assignment
- Predicted 1-year and 2-year survival estimates
- Transparent calculation logic showing how each variable contributed to the final score
- Risk stratification visual (color-coded low/intermediate/high risk band)
This transparency is especially valuable for teaching. When a fellow enters values and immediately sees the 5-point breakdown alongside clinical interpretation, the scoring logic becomes intuitive—strengthening understanding of hepatic reserve, portal hypertension severity, and prognosis.
4. Clinical Evidence and Validation
4.1 The Mathematical Foundation
The Child-Pugh Score uses point-based weighted aggregation rather than a regression model. Each parameter is assigned points based on empirically derived thresholds associated with survival outcomes:
Total Score = Bilirubin points + Albumin points + INR/PT points + Ascites points + Encephalopathy points
Each variable is scored independently (1–3 points); there are no multiplicative or interactive terms. This simplicity is a deliberate feature—the score was designed for rapid bedside calculation before the digital era—yet also a limitation. It does not account for dynamic variables like age, ethnicity, etiology of cirrhosis, or viral load, which influence outcomes independently of these five parameters.
4.2 Validation Evidence Across Populations
Original Cohort and Long-Term Validation: The score was validated in the original surgical population (Child & Turcotte, 1964; Pugh et al., 1972) and has been prospectively validated in thousands of cirrhotic patients across North America, Europe, and Asia. Large registry analyses confirm that Child-Pugh class stratifies mortality risk in decompensated cirrhosis, esophageal variceal bleeding, hepatic encephalopathy, and spontaneous bacterial peritonitis.
Asian Populations and Hepatitis B Cirrhosis: A substantial proportion of global cirrhosis burden stems from chronic hepatitis B, particularly in Asian regions. Recent validation studies in large Asian cohorts (including China, where hepatitis B remains endemic) confirm that Child-Pugh class predicts short-term (28-day, 90-day) and long-term (6-month, 1-year) mortality in both compensated and decompensated cirrhosis. The score performs equivalently across ethnic groups and HBV versus non-HBV populations when applied to the same clinical endpoints.
4.3 Comparative Performance Against Alternatives
The Child-Pugh Score is often compared to the Model for End-Stage Liver Disease (MELD) score. Contemporary evidence suggests:
- Child-Pugh excels in compensated cirrhosis (Class A/B) and stratifies risk intuitively for clinicians accustomed to its categorical framework
- MELD is marginally superior in short-term mortality prediction in decompensated cirrhosis and is now mandated for transplant priority allocation in many countries
- ALBI (Albumin-Bilirubin) score offers improved short-term prognostication (28–90 days) and may be particularly useful in Asian populations with HBV cirrhosis, but lacks the widespread clinical adoption and guideline endorsement of Child-Pugh
4.4 EASL and AASLD Guidance
Both the European Association for the Study of the Liver (EASL) and American Association for the Study of Liver Diseases (AASLD) continue to recognize Child-Pugh classification as a cornerstone of cirrhosis assessment, particularly for:
- Defining compensated versus decompensated disease
- Guiding variceal screening and prophylaxis
- Stratifying risk in PBC and PSC (with modified bilirubin thresholds for cholestatic diseases)
- Evaluating perioperative and transplant candidacy
4.5 Important Limitations and Caveats
No prognostic score perfectly predicts individual outcomes. Thoughtful clinicians should recognize:
- Static snapshot: Child-Pugh reflects disease severity at a single point in time. Serial rescoring (e.g., after diuretic therapy or acute decompensation reversal) is essential to track clinical trajectory.
- Does not account for etiology: A Class A patient with decompensating autoimmune hepatitis may deteriorate rapidly, whereas a stable Class A patient with well-controlled viral hepatitis may remain compensated for years.
- Age not incorporated: Older patients with identical Child-Pugh scores face higher surgical and transplant mortality than younger patients.
- Limited utility in HCC staging: While Child-Pugh class influences HCC treatment eligibility, integrated systems like BCLC or ALBI may be superior for HCC-specific decision-making.
- Subjective encephalopathy grading: Assigning hepatic encephalopathy grades (Grades 1–4) requires clinical judgment and can vary between observers.
5. How Our Calculator Works: Step-by-Step Workflow
5.1 Input and Data Entry
When you open the Child-Pugh calculator at /calculator/child-pugh-liver-cirrhosis-severity-score, you are presented with an intuitive, mobile-responsive form.
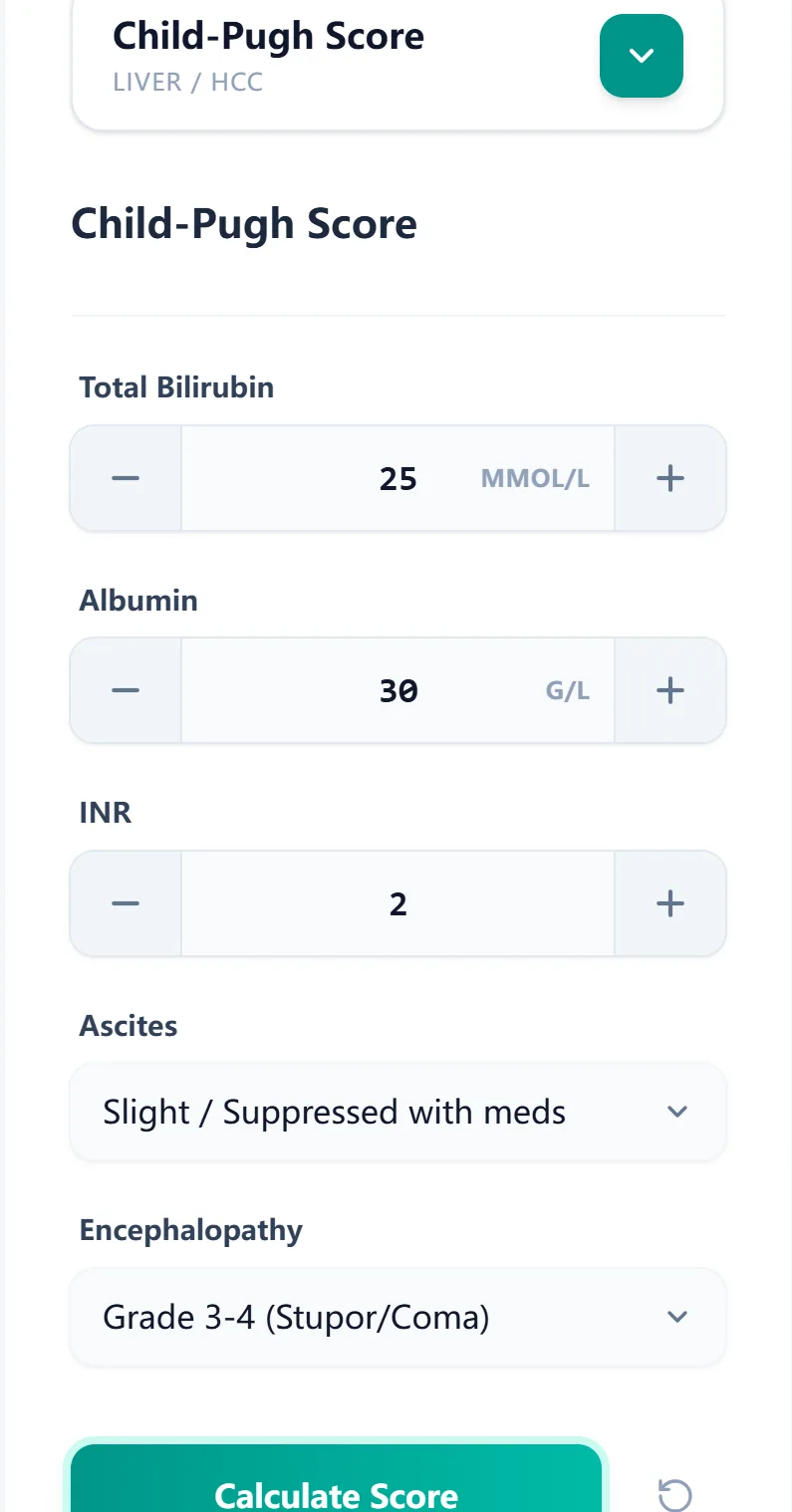
Each field is designed for rapid, error-resistant entry:
- Total Bilirubin: Enter numeric value; select unit (mg/dL or µmol/L).
- Serum Albumin: Enter numeric value; select unit (g/dL or g/L).
- INR or Prothrombin Time: Enter INR value directly (preferred) or prothrombin time in seconds.
- Ascites: Dropdown menu with clinically graded options (Absent, Slight, Moderate/Severe).
- Hepatic Encephalopathy: Dropdown with grades (Absent, Grade 1–2, Grade 3–4).
5.2 Algorithm and Score Calculation
Once you click "Calculate Score," the engine:
- Validates inputs: Ensures all fields are populated and values are within physiologic ranges.
- Maps values to points using the standard Child-Pugh thresholds.
- Sums total points and assigns class (A, B, or C).
- Retrieves prognostic data: Looks up 1-year and 2-year survival estimates.
- Renders results with full transparency.
5.3 Result Display and Interpretation
The result screen prominently displays:
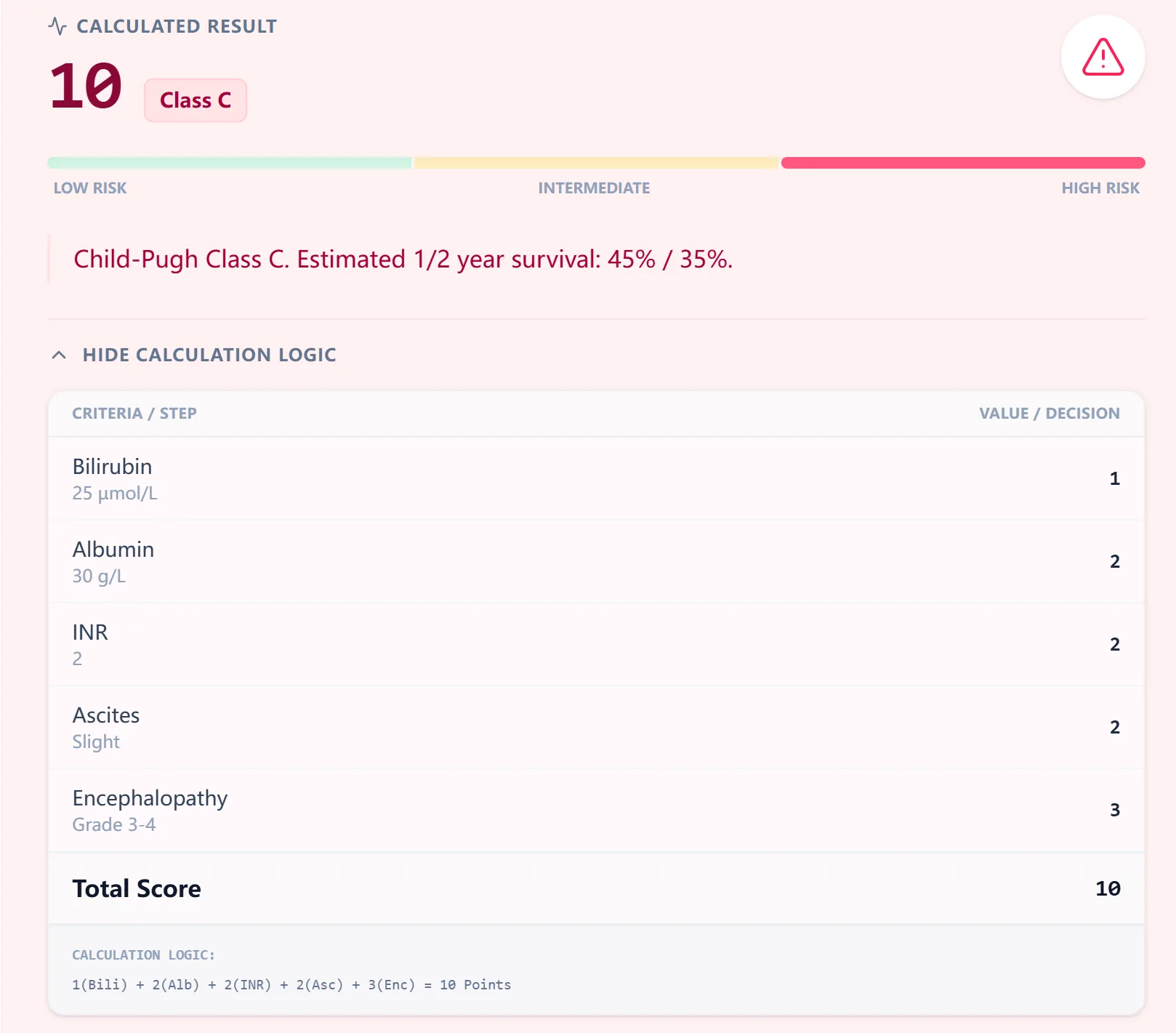
Key result fields:
- Total Score: Large, prominent display (e.g., "10 points")
- Class Assignment: Color badge (e.g., "Class C")
- 1-Year Survival Estimate: (e.g., "45%")
- Risk Stratification Visual: A gradient bar spanning low (green) to high (red) risk.
5.4 Calculation Logic Transparency
An expandable "Hide Calculation Logic" section displays the step-by-step computation:
5.4 Calculation Logic Transparency
An expandable "Hide Calculation Logic" section displays the step-by-step computation. Rather than a static table, the engine itemizes each clinical parameter to show exactly how the risk profile is built:
6. How the Platform Supports Clinical Care and Research
6.1 Routine Clinical Decision Support
The Child-Pugh calculator integrates seamlessly into daily hepatology practice. It assists with Point-of-Care Rounds, MDT Preparation, Treatment Decision Support, and Perioperative Risk Assessment.
6.2 Education and Simulation
OncoToolkit's calculator excels as a teaching tool for case-based learning and trainee self-assessment, ensuring all trainees learn cirrhosis risk stratification using the same evidence-grounded tool.
6.3 Clinical Research and Quality Improvement
For research and QI initiatives, the calculator's transparent logic is invaluable for Cohort Stratification, Outcome Dashboard Integration, Audit Monitoring, and Population Health analysis across entire health systems.
7. Clinical Context and Background
8. Frequently Asked Questions
When should you not use the Child-Pugh Score?
The Child-Pugh Score is designed for cirrhosis prognosis but is not appropriate for:
- Acute hepatitis without cirrhosis: Use King's College Criteria instead.
- Non-cirrhotic portal hypertension: Risk may be underestimated.
- HCC-specific staging: BCLC or ALBI-based systems are often superior.
- Acute decompensation: Confirm underlying chronic disease first.
How does the Child-Pugh Score differ from the MELD Score?
While both systems assess liver dysfunction, they serve distinct clinical roles. The Child-Pugh Score is a point-based system (ranging 5–15) that categorizes patients into Classes A, B, or C. It relies on five variables—Bilirubin, Albumin, INR, Ascites, and Encephalopathy—making it highly effective for staging compensated cirrhosis and assessing general bedside prognosis. However, it does not incorporate renal function, which can be a critical blind spot in acute care.
In contrast, the MELD Score (Model for End-Stage Liver Disease) utilizes a continuous regression formula resulting in a score from 6 to 40. It prioritizes objective laboratory data—Bilirubin, INR, and Creatinine (with optional Sodium in MELD-Na)—to predict short-term mortality. Because MELD explicitly includes Creatinine, it captures the risk of hepatorenal syndrome, making it the superior tool for determining transplant urgency and organ allocation priority in decompensated cases.
What is the most common mistake when calculating the score?
- Confusing PT and INR: Entering PT seconds into an INR field.
- Misgrading ascites: Using lab markers alone rather than physical exam/imaging.
- Undergrading encephalopathy: Missing Grade 1–2 confusion during bedside assessment.
Is the score validated in Asian populations with HBV?
Yes, extensively. Large studies in China and South Korea confirm that Child-Pugh class stratifies mortality risk in HBV cirrhosis (area under ROC typically 0.75–0.85). It performs equally well with or without concurrent HCV.
How often should you recalculate the Child-Pugh Score?
- Class A: Annually.
- Class B: Every 3–6 months.
- Class C: Monthly or more frequently if acute decompensation occurs.
9. Summary of Clinical Utility
The Child-Pugh Score remains the foundation of cirrhosis risk stratification globally. It is endorsed by AASLD and EASL, validated across Western and Asian populations, and directly informs transplant prioritization and perioperative risk assessment.
Our mobile-optimized calculator eliminates manual calculation barriers. By delivering instantaneous, transparent Child-Pugh classification alongside survival estimates, OncoToolkit helps you practice faster, teach more effectively, and support research-grade cohort analysis—all from point of care.
Ready to Simplify Your Cirrhosis Risk Assessment?
Use the Child-Pugh Calculator
References
- Child CG, Turcotte JG. Surgery and portal hypertension. Major Probl Clin Surg. 1964;1:1-85.
- Pugh RN, Murray-Lyon IM, Dawson JL, Pietroni MC, Williams R. Transection of the oesophagus for bleeding oesophageal varices. Br J Surg. 1973;60(8):646-9.
- Lu J, et al. Child-Pugh Score and Prognosis in Liver Cirrhosis. Source
- Non-virological factors and HBV HCC risk. Source
- Child-Pugh 7 Subset Analysis. Source
- EASL Clinical Practice Guidelines: Decompensated Cirrhosis. Source
- Validation in Large Cohorts. Source
- StatPearls: Child-Pugh Classification. Source
- Clinical Decision Support and CTP. Source
- Medical Calculators: CTP Score. Source
- Child-Pugh score on Wikipedia. Source
- Comparative Studies on Liver Failure. Source
- SPS: Calculating Child-Pugh. Source
- Hepatology Validation Studies. Source
- Cleveland Clinic on CTP. Source
- Asian Population Validation (HBV). Source