Gail Model (Relative Risk) Breast Cancer Risk Calculator
Estimate 5-year and lifetime breast cancer risk with the Gail Model (Relative Risk) and get treatment-oriented interpretation in seconds using the OncoToolkit calculator.
Quick Navigation
1. Introduction
Breast surgical oncologists and breast surgeons are increasingly expected to practice risk-adapted screening and prevention, yet formal risk models are still underused in day-to-day clinics. The Gail Model (Relative Risk), or Breast Cancer Risk Assessment Tool (BCRAT), remains one of the most widely recognized instruments for estimating a woman’s probability of developing invasive breast cancer over the next 5 years and over her lifetime. At OncoToolkit, we’ve built a streamlined Gail Model (Relative Risk) calculator that transforms this complex statistical model into a fast, point-of-care decision support tool tailored to busy breast practices.1, 2, 3, 4, 5, 6
In what follows, we’ll review how the Gail Model works, why it matters for breast surgeons, what the evidence says about its performance, and how our calculator integrates the math with clinically meaningful thresholds. We’ll also highlight practical tips, edge cases, and ways to incorporate this tool into MDTs, high-risk clinics, and research.2, 3, 7, 8
2. Understanding the Gail Model (BCRAT) for Breast Cancer Risk Assessment
The Gail Model was originally developed to project individualized breast cancer risk for women undergoing regular screening, using logistic regression models built on large cohort data from the Breast Cancer Detection Demonstration Project. It combines a small set of easily collected clinical variables with age-specific breast cancer incidence rates to estimate absolute risk. The relative risk component expresses how a particular constellation of risk factors compares with the “average” risk for a woman of the same age in the general population.3, 4, 9, 10
2.1 Clinical Variables Included in the Gail Model
In its commonly used form, the Gail Model incorporates:9, 10, 3
- Current age
- Age at menarche
- Age at first live birth (including nulliparity)
- Number of first-degree relatives with breast cancer (mother, sisters, daughters)
- Number of previous benign breast biopsies
- Presence or absence of atypical hyperplasia in any biopsy
OncoToolkit’s Gail Model (Relative Risk) calculator focuses the user interface on the variables that shape the relative risk term—age at menarche, age at first birth, number of biopsies, presence of atypical hyperplasia, and number of affected first-degree relatives—while handling age and background incidence in the backend. The result is a clean clinical form that matches the way breast surgeons collect history, without exposing users to the complexity of the underlying equations.5, 10, 11, 3
2.2 What the Gail Model Predicts: 5-Year and Lifetime Risk
The model provides two main outputs:4, 3
- 5-year absolute risk of developing invasive breast cancer
- Lifetime risk (usually to age 90) of invasive breast cancer
The relative risk acts as a multiplier on age-specific baseline hazard, so a woman with a relative risk of 2.0 has approximately double the risk of an average woman of the same age, although absolute risk still depends on her starting baseline. For clinical decision making, thresholds such as 1.67% 5-year risk (and, in more recent work, 3% 5-year risk) have been used to define women at increased risk who should be offered chemoprevention.10, 12, 13, 14, 4
3. The Clinical Importance of the Gail Model in Breast Surgical Oncology
3.1 Linking Risk Assessment to Real-World Clinical Decisions
In the hands of a breast surgeon, the Gail Model informs several concrete questions:
- Should I offer endocrine risk-reduction? A 5-year BCRAT (Gail) risk ≥1.67% was used to define “increased risk” in landmark tamoxifen and raloxifene prevention trials and in FDA approvals for these agents. Analyses suggest that higher thresholds (e.g., ≥3% 5-year risk) may better balance benefit and toxicity for modern practice.12, 13, 14
- Does this patient qualify for enhanced screening? Women with substantially elevated risk, especially when lifetime risk exceeds ~20%, are candidates for supplemental MRI or more frequent surveillance in many high-risk protocols.8, 1, 12
- How do I prioritize genetics or high-risk clinic referrals? Although not a hereditary cancer model, Gail-derived risk helps contextualize women with moderate combinations of common risk factors who may not meet strict pedigree-based criteria but clearly sit above “average” risk.1, 2
3.2 Pain Points of Manual Risk Calculation
In paper or “mental math” form, the Gail Model is difficult to use consistently:
- Age- and race-specific baseline incidence tables are not easily memorized.3, 4
- Multiple categorical variables interact multiplicatively, which makes manual estimation unreliable.9, 10
- Textbook examples rarely map directly onto nuanced clinical scenarios, leading to underuse or reliance on informal heuristics.7, 15
3.3 How Our Digital Tool Alleviates Calculator Fatigue
On our platform, the Gail Model (Relative Risk) calculator is:
- Single-screen and mobile-responsive, so it can be opened during MDTs, in the operating room holding bay, or at the bedside.6, 11
- Optimized for dropdown selection, reducing keystrokes and transcription errors and allowing a fellow or nurse to complete the form while you take the rest of the history.11
- Integrated with clear interpretive bands, so that you immediately see whether the patient is at average, above-average, or high risk and what that implies for chemoprevention and imaging.16, 6, 12
4. Evidence-Based Validation and Performance of the Gail Model
4.1 The Mathematical Foundation of Relative Risk
Under the hood, the Gail Model uses multivariable logistic regression to generate age-specific relative risks for combinations of risk factors, derived from large screening cohorts. Each risk factor is translated into a categorical term with a coefficient; conceptually, each factor contributes a multiplier such as RR_menarche, RR_first_birth, RR_biopsies, RR_atypia, and RR_relatives.4, 10, 3, 9
The individual’s overall relative risk is the product of these components:10, 9
RR = RR_menarche x RR_first_birth x RR_biopsies x RR_atypia x RR_relatives
This relative risk is then applied to age‑specific incidence rates, adjusted for competing mortality, to obtain absolute risk over a period t:3, 4
Absolute Risk (0, t) = Integral from 0 to t of [baseline hazard λ₀(a)] × RR × [survival function S(a)] da
where λ₀(a) is the baseline age‑specific hazard and S(a) is the survival function reflecting the probability of being alive and cancer‑free at age a. In digital implementations, these integrals are precalculated or approximated, enabling instant outputs once the risk factors are known.17, 4, 3
4.2 Typical Validation Cohorts and Model Performance
The Gail Model has been studied in a wide range of populations:
- Original U.S. cohorts: Early validation in the placebo arm of the Breast Cancer Prevention Trial and other U.S. cohorts showed good calibration between predicted and observed breast cancer incidence, though with some over‑ or under‑prediction when incidence rates changed over time.18, 19
- Australian screening cohorts: A prospective validation in more than 40,000 Australian women demonstrated that the NCI BCRAT had reasonable calibration and that observed invasive breast cancer incidence increased across Gail risk quintiles.20, 21
- Spanish population studies: A population‑based cohort of Spanish women showed that recalibration of the Gail Model using local incidence data improved calibration compared with the original U.S. parameters.15, 22
- Asian and multiethnic cohorts: Validation studies in Asian women and other non‑U.S. populations have reported variable calibration, often with overestimation of risk unless local adjustments are made.23, 7, 9
5. Navigating the OncoToolkit Gail Model Calculator Interface
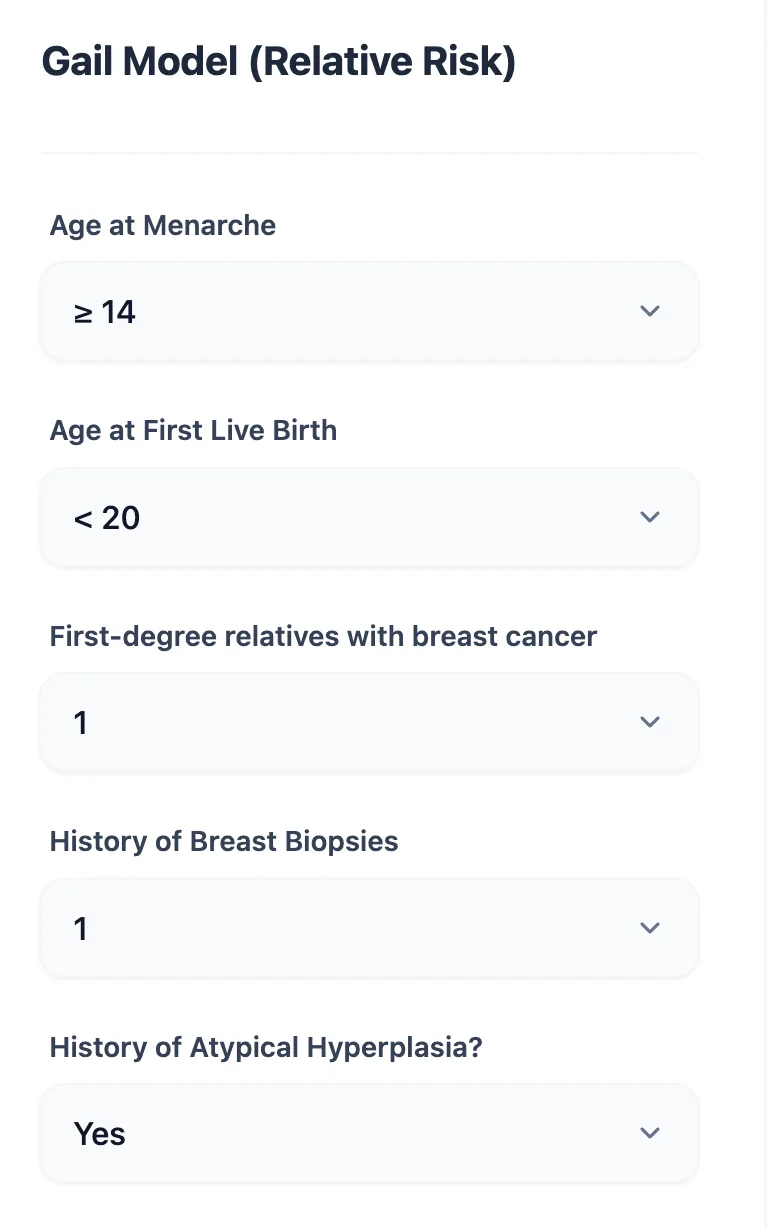
5.1 Input Form: Mirroring the Clinic History
Figure 1. The input form uses structured dropdowns for each variable—age at menarche, age at first live birth, number of first‑degree relatives, benign biopsies, and atypical hyperplasia—allowing rapid, error‑resistant data entry in clinic.11
5.2 Reference Bands and Defined Risk Thresholds
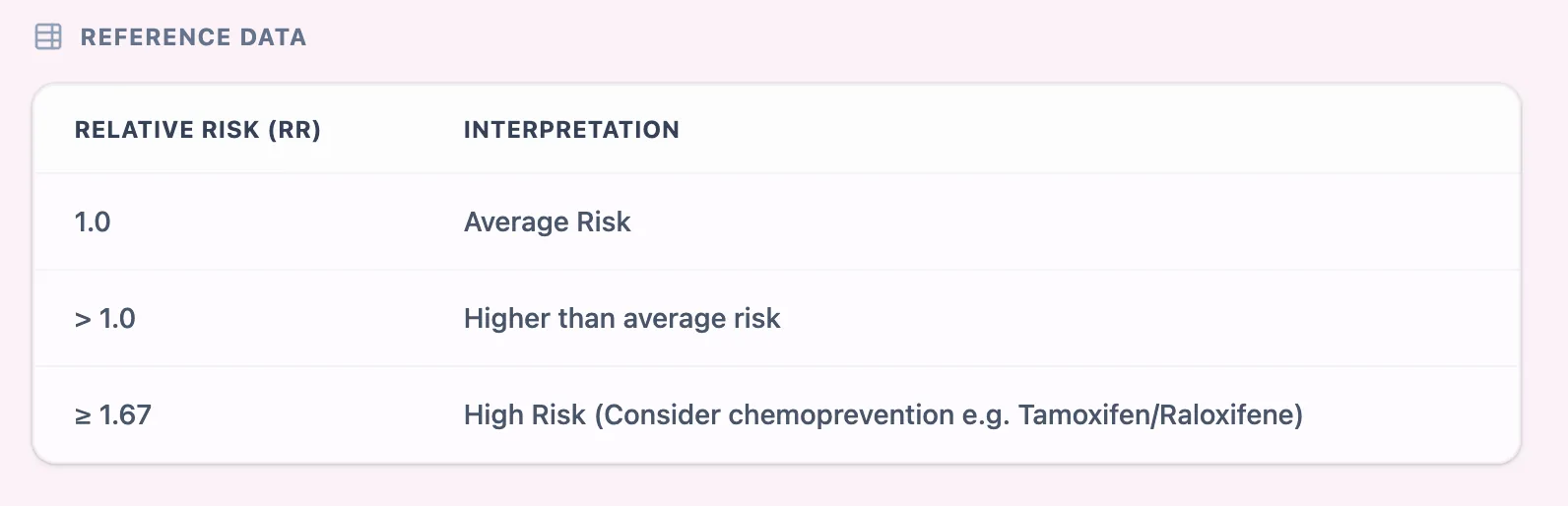
Figure 2. A clear reference table translates numeric relative risk into qualitative bands, with RR = 1.0 indicating average risk, RR > 1.0 indicating above‑average risk, and RR ≥ 1.67 highlighting high risk where chemoprevention and intensified screening should be considered.13, 16, 12
5.3 Result View: Actionable Interpretation at a Glance
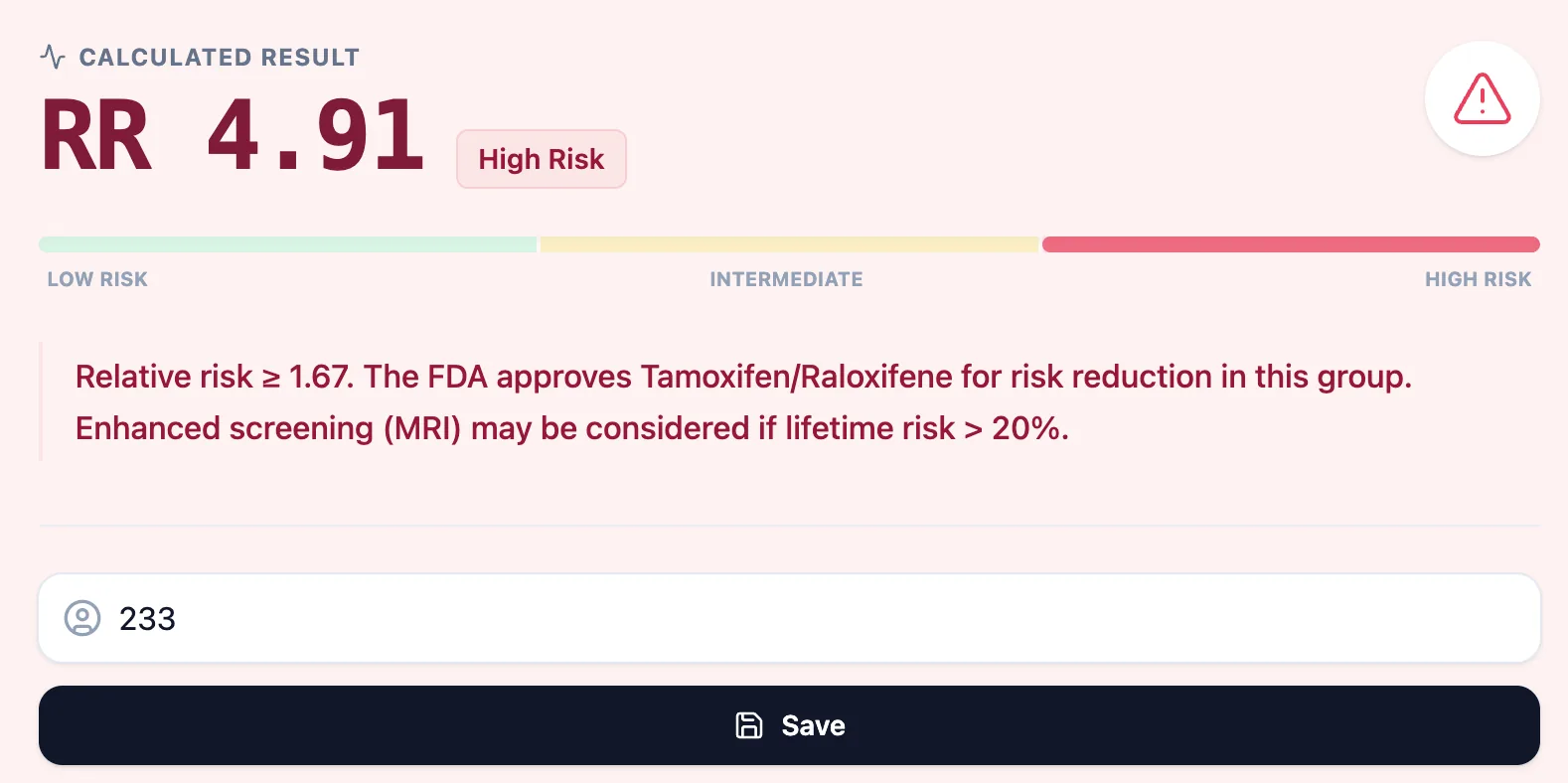
Figure 3. The result page shows the numeric relative risk, a color‑coded bar spanning low to high risk, and a concise narrative statement linking high risk to FDA‑approved endocrine risk‑reduction options and potential indications for enhanced imaging.6, 12
5.4 Embedded Clinical Context and Evidence
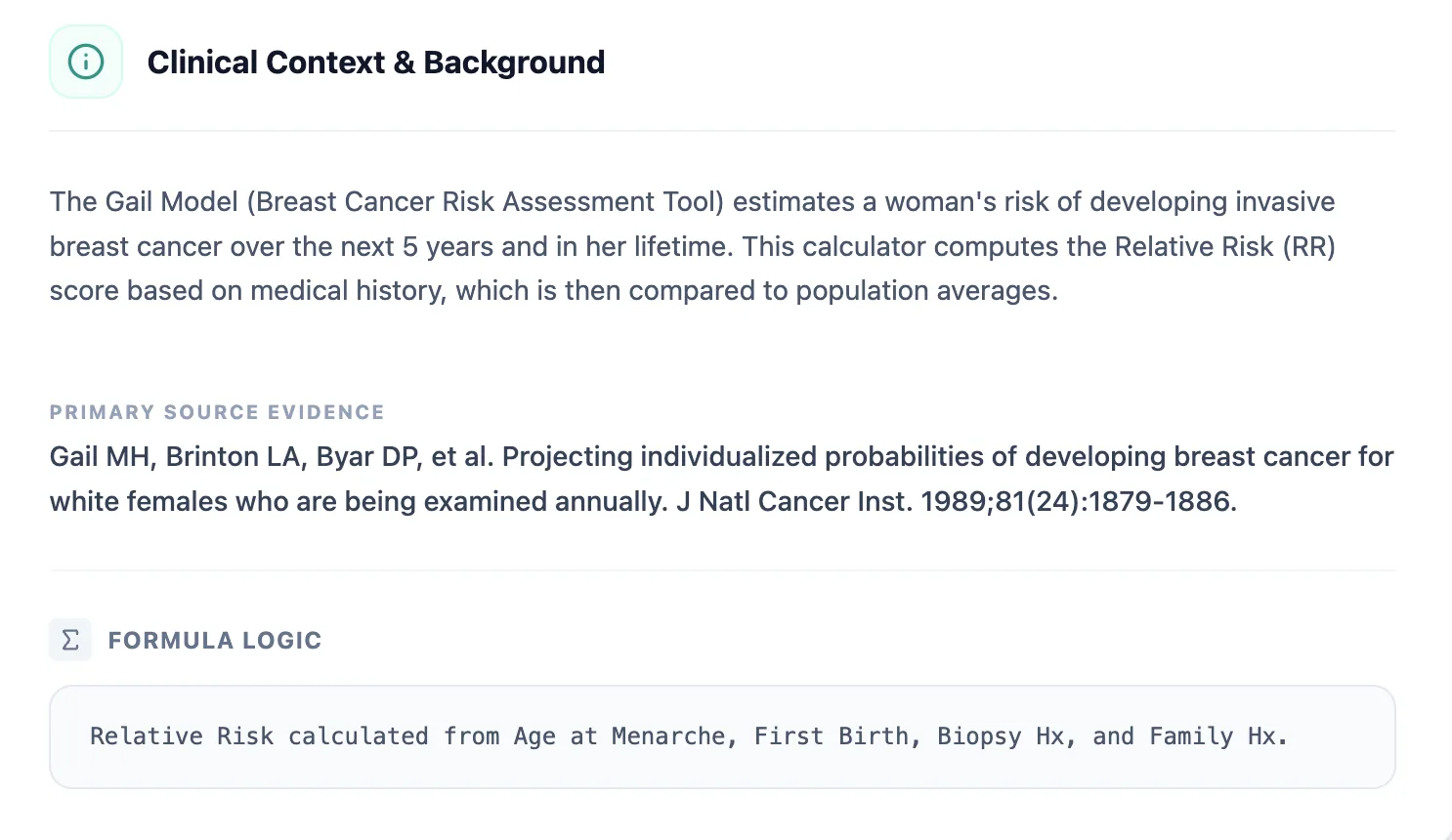
Figure 4. The clinical background section summarizes the purpose of the Gail Model, the core risk factors, and the primary source evidence, supporting transparency and trainee learning.5
6. Empowering Clinical Care and Research with Digital Risk Assessment
6.1 Routine Clinical Decision Support
In day-to-day practice, the Gail Model calculator can be integrated at multiple touchpoints:
- First high-risk visit: Use the calculator during the first consultation for women referred with atypia, multiple affected relatives, or other concerning histories to anchor discussions about their baseline risk.8, 1
- Screening strategy review: When patients are unsure whether they qualify for MRI or intensified follow-up, calculating Gail risk (alongside other models if needed) can make the pathway transparent and reproducible.1, 12
- Chemoprevention clinics: For women being seen to discuss tamoxifen, raloxifene, or aromatase inhibitor prophylaxis, having a quantifiable risk that crosses the relevant threshold helps frame benefit–risk discussions.14, 12
7. Clinical FAQ: Common Questions on Gail Model Application
Can the Gail Model (Relative Risk) be used for BRCA-positive patients or those with very strong hereditary patterns?
No. The Gail Model was not designed for women with known high-penetrance mutations such as BRCA1/2 or TP53 or with striking hereditary patterns. In those situations, models such as Tyrer–Cuzick or BOADICEA are more appropriate.7, 15, 3, 4
8. Call to Action: Integrate the Gail Model Calculator Into Your Workflow
To start using the Gail Model (Relative Risk) in your practice, visit and bookmark: https://oncotoolkit.com/calculator/gail-model-breast.3
Ready to Simplify Your Breast Risk Assessments?
Calculate 5-year and lifetime risk instantly with our optimized Gail Model tool.
Access the Gail Model Calculator
Free to use for clinicians. No registration required.
References
- Susan G. Komen. Understanding Risks: Gail Method. Source
- UVA Health. Gail Model Risk Assessment. Source
- National Cancer Institute. Breast Cancer Risk Assessment Tool (BCRAT). Source
- National Cancer Institute. About the BCRAT. Source
- OncoToolkit. GAIL-calculator-clinical-background.jpg.
- OncoToolkit. GAIL-calculated-result-example.jpg.
- The University of Hong Kong. Validation of Breast Cancer Risk Models. Source
- University of Michigan Health West. Gail Model High-Risk Breast Assessment. Source
- PMC. Development and Validation of the Gail Model. Source
- MDApp. Gail Model for Breast Cancer Risk Calculator. Source
- OncoToolkit. GAIL-calculator-input-data-submission-form.jpg.
- NCBI Bookshelf. Medications for Breast Cancer Risk Reduction. Source
- Nature NPJ Breast Cancer. Breast Cancer Risk Thresholds. Source
- USPSTF. Evidence Summary: Medications for Risk Reduction. Source
- PMC. Evaluation of the Gail Model in Spanish Women. Source
- OncoToolkit. GAIL-calculator-reference-table.jpg.
- NCI DCEG. Risk Assessment SAS Macros. Source
- Journal of Clinical Oncology. Calibration of the Gail Model. Source
- Washington University. Effect of Changing Incidence on Calibration. Source
- DOAJ. Gail Model Validation in Australian Cohorts. Source
- PMC. Prospective Validation of the BCRAT. Source
- PubMed. Recalibration of the Gail Model. Source
- PMC. Performance of Breast Cancer Risk Models in Asian Women. Source